

Anal cancer in high-income countries: Increasing burden of disease
- PMID: 30339668
- PMCID: PMC6195278
- DOI: 10.1371/journal.pone.0205105
Anal cancer in high-income countries: Increasing burden of disease
Erratum in
-
Correction: Anal cancer in high-income countries: Increasing burden of disease.PLoS One. 2019 May 8;14(5):e0216884. doi: 10.1371/journal.pone.0216884. eCollection 2019. PLoS One. 2019. PMID: 31067265 Free PMC article.
Abstract
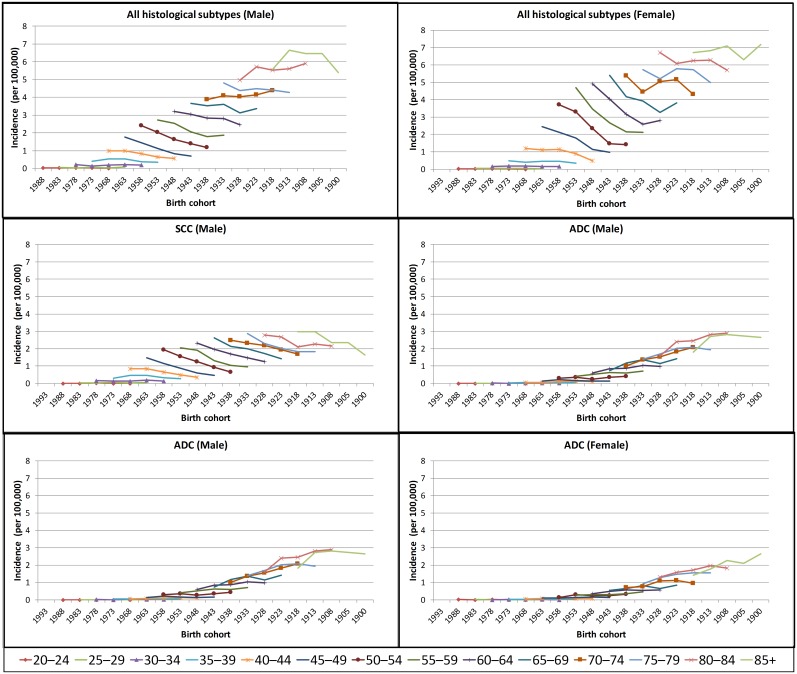
Background: Previous studies have reported that anal cancer incidence has increased in individual countries; however, age-specific trends were not examined in detail. This study describes pooled and country-specific anal cancer incidence trends by sex, age (all ages, <60 and 60+ years) and histological subtype (all subtypes, squamous cell carcinoma [SCC] and adenocarcinoma [ADC]).
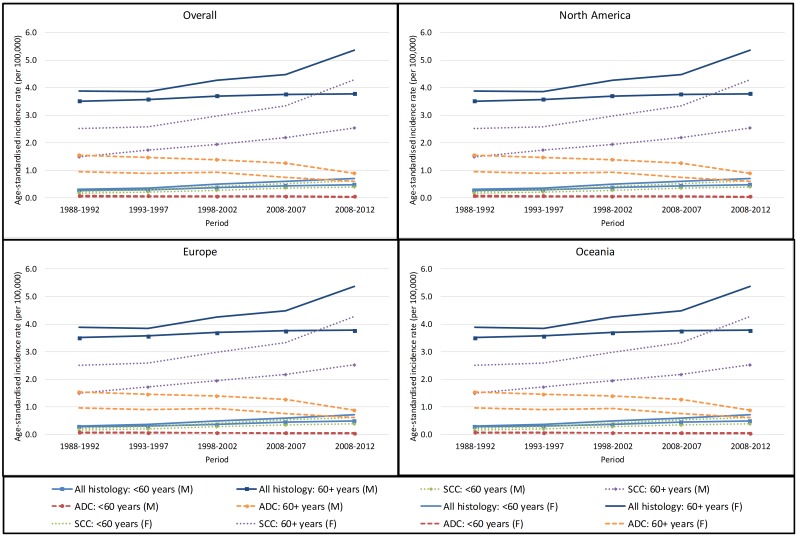
Methods: Five-year incidence and population-at-risk data were obtained from IARC's Cancer Incidence in Five Continents for the years 1988-1992 to 2008-2012. The standardised rate ratios (SRRs) for 2008-2012 vs 1988-1992 and the 5-year average percent change (AvPC) during the period were used to assess changes in the age-standardised incidence rates.
Results: During the study period, there were significant increases in the incidence of SCC in both men and women of all age groups with significant increasing trend, and these increases were highest in those aged <60 years (SRR = 2.34 [95% CI:2.11-2.58] in men and SRR = 2.76 [95% CI:2.54-3.00] in women). By contrast, there were significant decreases in the incidence of ADC in men and women of all ages (SRR = 0.60 [95% CI:0.54-0.67]) and (SRR = 0.63 [95% CI:0.56-0.71], respectively), with similar decreases in those aged <60 years and 60+ years. These competing trends still resulted in significant increases in the overall incidence of anal cancer in men and women of all ages groups with significant increasing trend. The SRRs in men of all ages, <60 years and 60+ years were 1.35 (95% CI:1.28-1.42), 1.77 (95% CI:1.62-1.92) and 1.08 (95% CI:1.00-1.15), respectively. The corresponding SRRs in women were 1.75 (95% CI:1.67-1.83), 2.31 (95% CI:2.14-2.48) and 1.38 (95% CI 1.31-1.46), respectively.
Conclusion: Increases in the incidence of anal SCC has driven an overall increase in anal cancer incidence; this may be associated with changing sexual behaviours and increasing levels of HPV exposure in younger cohorts. The findings further reinforce the importance of HPV vaccination.
Conflict of interest statement
KC is co-Principal Investigator of an unrelated investigator-initiated trial of cytology and primary HPV screening for cervical cancer in Australia (Compass; ACTRN12613001207707 and NCT02328872), which is conducted and funded by the Victorian Cytology Service. The Victorian Cytology Service has received equipment and a funding contribution for the Compass trial from Roche Molecular Systems and Ventana. KC is also a Principal Investigator of Compass in New Zealand (Compass NZ; ACTRN12614000714684), which is conducted and funded by Diagnostic Medlab, now Auckland District Health Board. Diagnostic Medlab received equipment and a funding contribution for the Compass trial from Roche Molecular Systems. Neither KC nor her institution on her behalf (Cancer Council NSW) receive direct or indirect funding from industry for Compass Australia or NZ, or any other project. KC receives salary support from NHMRC Australia (Career Development Fellowship APP1082989). This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Bruni L, Barrionuevo-Rosas L, Albero G, Aldea M, Serrano B, Valencia S, et al. ICO Information Centre on HPV and Cancer (HPV Information Centre). Human Papillomavirus and Related Diseases in the World. Summary Report 2016-02-25.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
