

Regression techniques employing feature selection to predict clinical outcomes in stroke
- PMID: 30339669
- PMCID: PMC6195279
- DOI: 10.1371/journal.pone.0205639
Regression techniques employing feature selection to predict clinical outcomes in stroke
Abstract
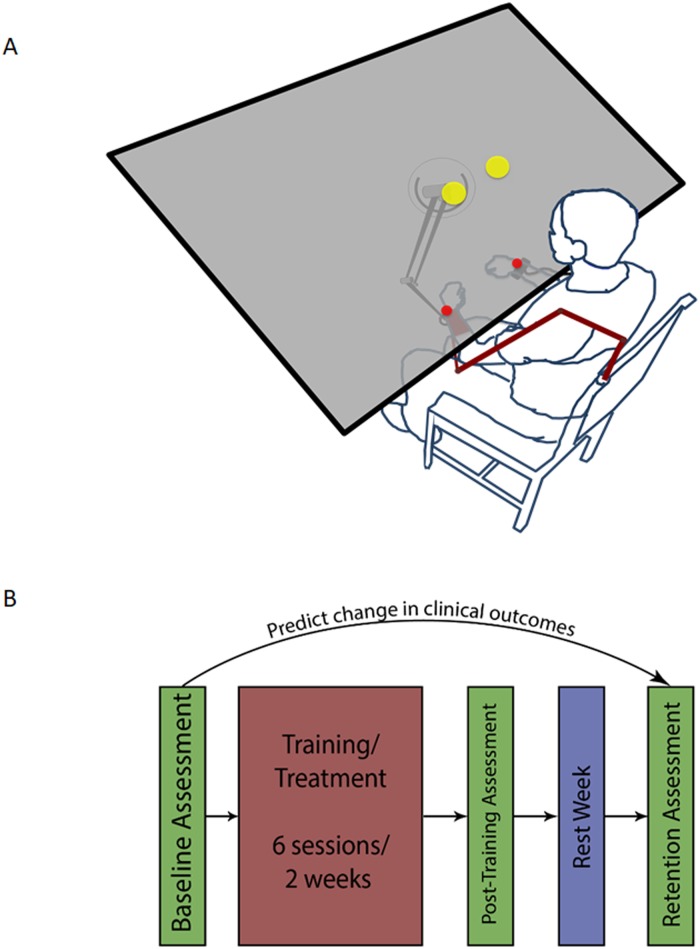
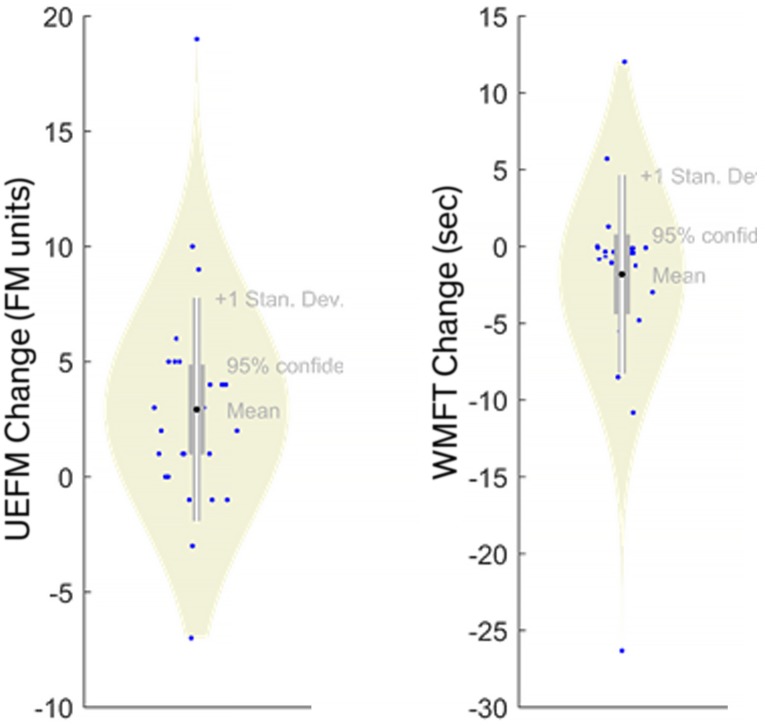
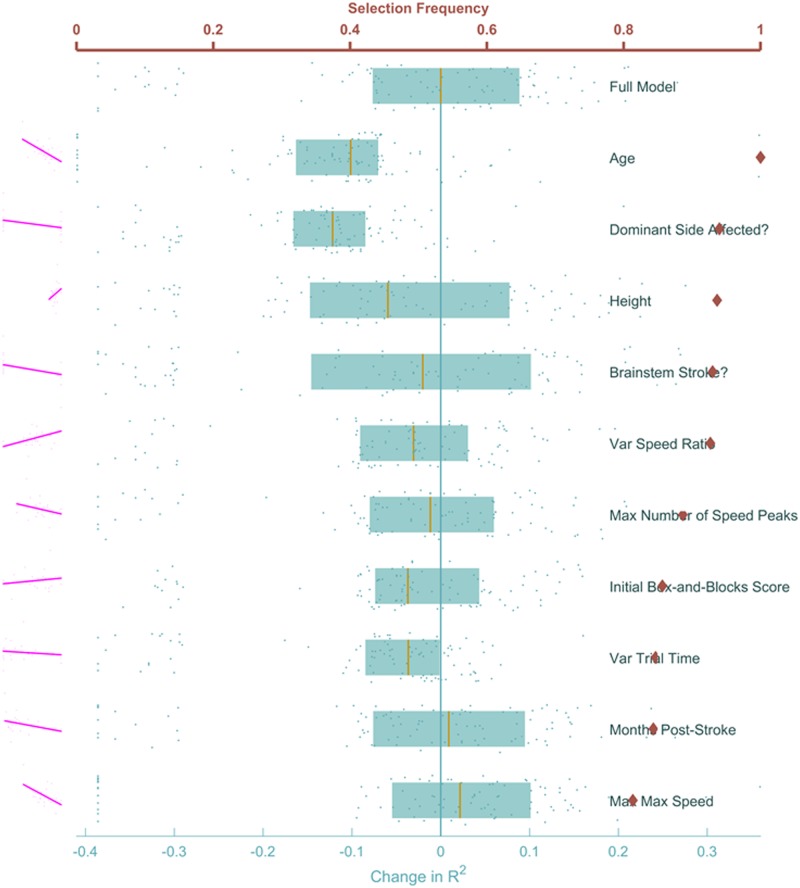
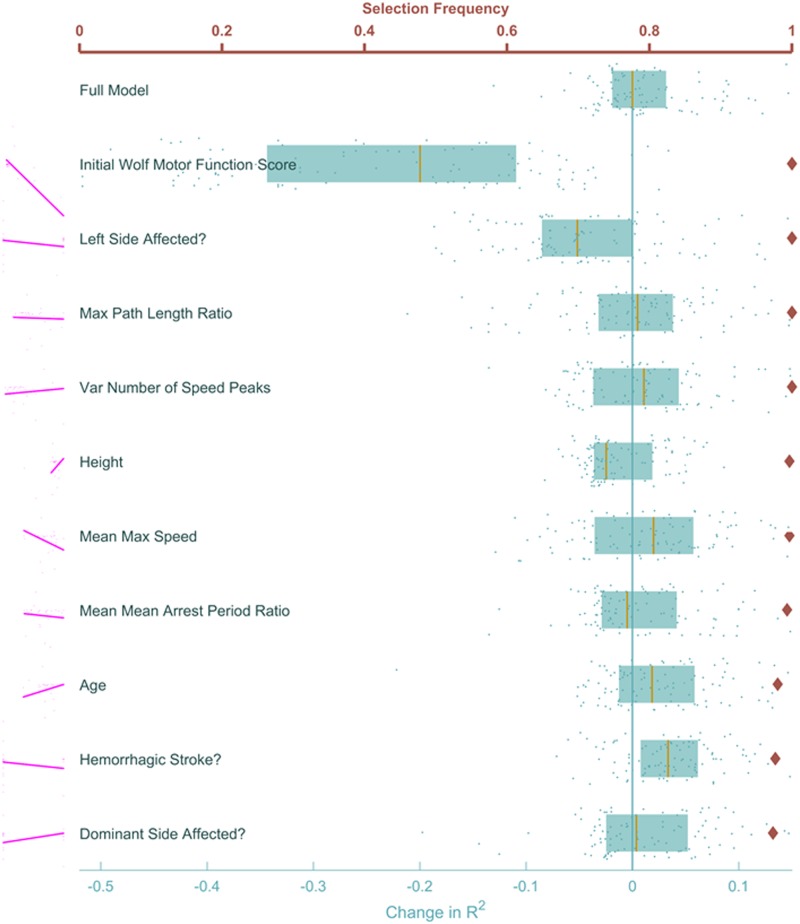
It is not fully clear which measurable factors can reliably predict chronic stroke patients' recovery of motor ability. In this analysis, we investigate the impact of patient demographic characteristics, movement features, and a three-week upper-extremity intervention on the post-treatment change in two widely used clinical outcomes-the Upper Extremity portion of the Fugl-Meyer and the Wolf Motor Function Test. Models based on LASSO, which in validation tests account for 65% and 86% of the variability in Fugl-Meyer and Wolf, respectively, were used to identify the set of salient demographic and movement features. We found that age, affected limb, and several measures describing the patient's ability to efficiently direct motions with a single burst of speed were the most consequential in predicting clinical recovery. On the other hand, the upper-extremity intervention was not a significant predictor of recovery. Beyond a simple prognostic tool, these results suggest that focusing therapy on the more important features is likely to improve recovery. Such validation-intensive methods are a novel approach to determining the relative importance of patient-specific metrics and may help guide the design of customized therapy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Platz T, Pinkowski C, van Wijck F, Kim IH, Di Bella P, Johnson G. Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: a multicentre study. Clinical Rehabilitation. 2005;19(4):404–411. 10.1191/0269215505cr832oa - DOI - PubMed
-
- Fugl-Meyer AR, Jääskö L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scandinavian journal of rehabilitation medicine. 1974;7(1):13–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
