

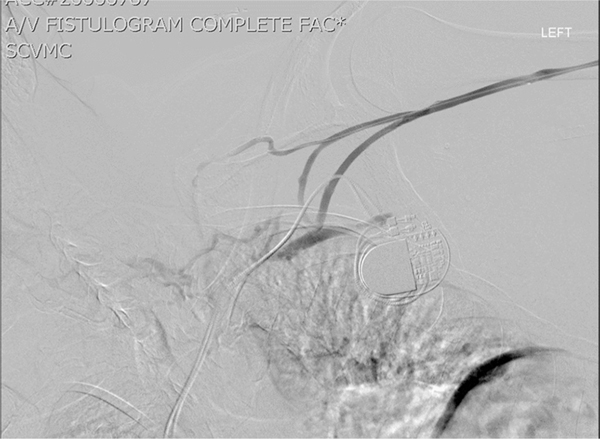
Arteriovenous Fistula and Graft Construction in Patients with Implantable Cardiac Devices: Does Side Matter?
- PMID: 30339901
- PMCID: PMC8439285
- DOI: 10.1016/j.avsg.2018.10.003
Arteriovenous Fistula and Graft Construction in Patients with Implantable Cardiac Devices: Does Side Matter?
Abstract
Background: Limited reports have documented the effect cardiac implantable electronic devices (CIEDs) have on arteriovenous (AV) access patency. Current recommendations suggest placing the access on the contralateral side of the CIEDs, as there is concern for increased central venous stenosis and access failure. The goal of this study is to review our single-center AV access patency rates for dialysis patients with an ipsilateral or contralateral side CIED.
Methods: A retrospective review was performed from 2008 to 2016 at a single institution identifying all patients who have received a CIED and the diagnosis of end-stage renal disease (ESRD). Medical records were queried to identify each patient's dialysis access and whether it was ipsilateral or contralateral to the CIED. Primary outcomes of study were primary and secondary patency rates.
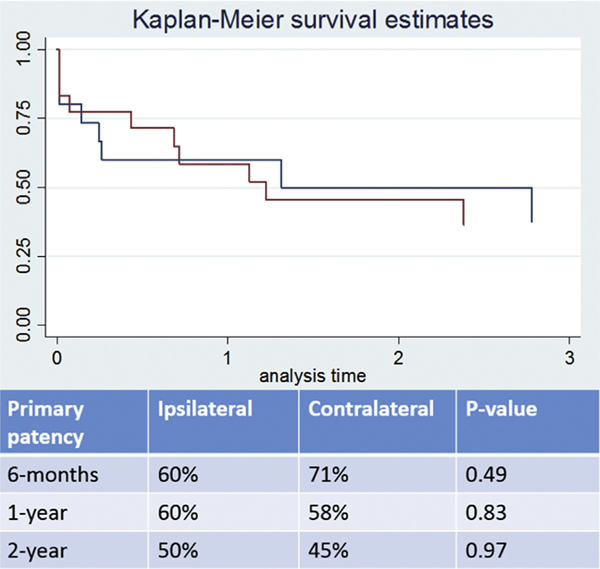
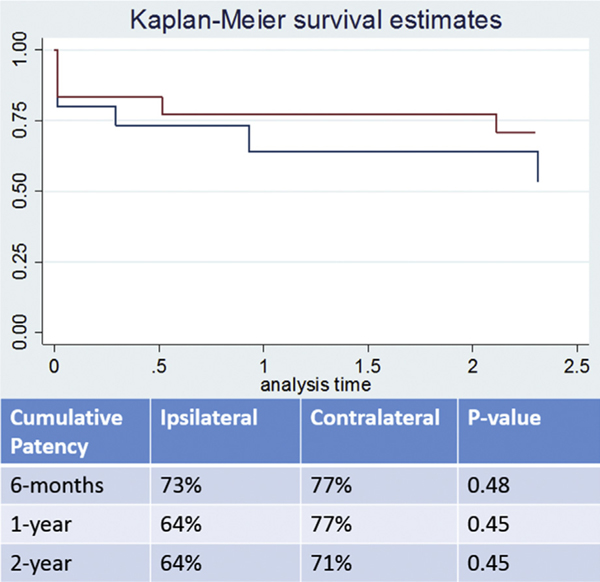
Results: A total of 44 patients were identified to have ESRD and CIED. Of these patients, 28 patients with fistulas or grafts (13 ipsilateral and 15 contralateral) had follow-up with regards to their AV access. There were 3 primary failures in both groups. For patients who had the CIED placed after already starting the dialysis, patency was based on when the cardiac device was implanted. Primary patency for ipsilateral and contralateral access was 20.2 and 22.2 months, respectively. With secondary interventions, ipsilateral and contralateral mean patency was 39 and 48.8 months, respectively. Six-month and 1-year primary patency for arteriovenous fistula or arteriovenous graft on patients with ipsilateral access was 69.2% and 53.8%, respectively. Ipsilateral 1-year cumulative patency was 39 months.
Conclusions: CIED may lead to stenosis or occlusion to one's AV access; however, primary assisted and secondary patency rates are still acceptable at 6 months and 1 year compared to Kidney Disease Outcomes Quality Initiative guidelines. Despite a CIED, a surgeon's algorithm should not lead to the abandonment of an ipsilateral access if the central venous system is patent.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures
References
-
- Saad TF, Weiner HL. Venous hemodialysis catheters and cardiac implantable electronic devices: avoiding a high-risk combination. Semin Dial 2017;30:187–92. - PubMed
-
- Saad TF, Hentschel DM, Koplan B, et al., ASDIN Clinical Practice Committee Workgroup. Cardiovascular implantable electronic device leads in CKD and ESRD patients: review and recommendations for practice. Semin Dial 2013;26: 114–23. - PubMed
-
- Herzog CA, Li S, Weinhandl ED, et al.Survival of dialysis patients after cardiac arrest and the impact of implantable cardioverter defibrillators. Kidney Int 2005;68:818–25. - PubMed
-
- Sakhuja R, McLaughlin GC, Thakur R, et al.Meta-analysis of mortality in dialysis patients with an implantable cardioverter defibrillator. Am J Cardiol 2009;103:735–41. - PubMed
-
- Oginosawa Y, Abe H, Nakashima Y. The incidence and risk factors for venous obstruction after implantation of transvenous pacing leads. Pacing Clin Electrophysiol 2002;25: 1605–11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
