

Estrogen is involved in hemangioma regression associated with mast cells
- PMID: 30340617
- PMCID: PMC6195721
- DOI: 10.1186/s13023-018-0928-x
Estrogen is involved in hemangioma regression associated with mast cells
Abstract
Background: Estrogen plays a role in infantile hemangioma (IH) development, but the underlying mechanism remains unclear. This study aimed to assess estrogen and estrogen receptor (ER) localization and expression levels in IH. In addition, the unexpected relationship between mast cells (MCs) and estrogen in human IH was discussed.
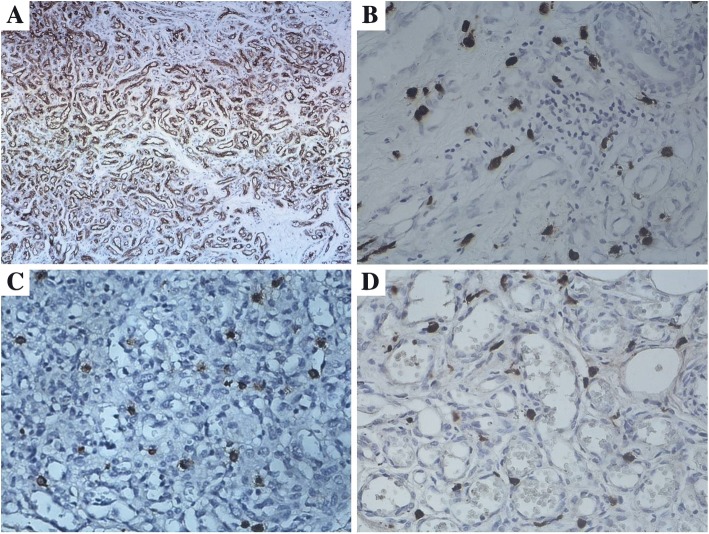
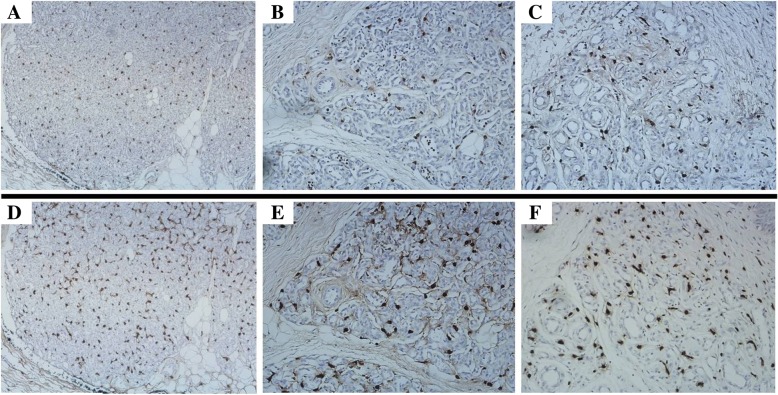
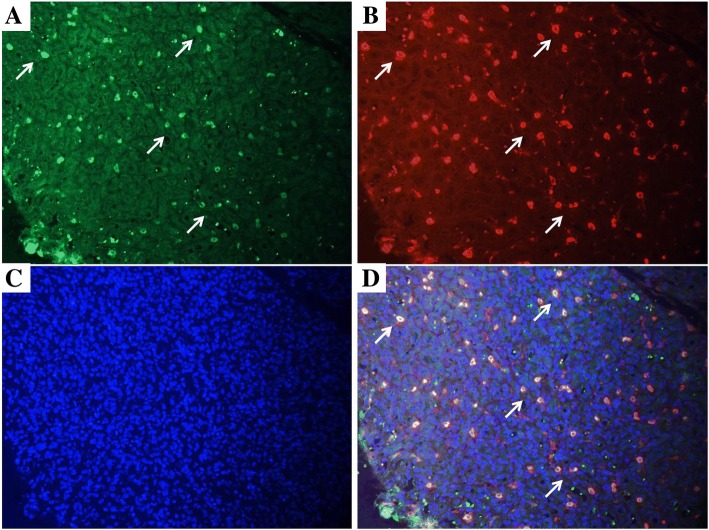
Methods: IH (n = 29), vascular malformation (VMs, n = 33) and normal skin (n = 15) specimens were assessed. IH was classified into proliferative (n = 9; age, 3.56 ± 1.01 months), early involuting (n = 10; age, 8.90 ± 2.69 months) and late involuting (n = 10; age, 20.10 ± 4.93 months) groups. Estradiol (E2), ER-a, ER-β, and tryptase (MC marker) levels were determined immunohistochemically and/or by double immunofluorescence staining. Quantification and localization of tryptase, ER-a, and E2 were assessed for each specimen.
Results: ER-a, E2, and tryptase were expressed in the cytoplasm and nucleus of MCs in IH. The IH specimens showed significantly more tryptase, ER-a, and E2 positive MCs (30.6 ± 12.7, 9.7 ± 5.6, and 19.8 ± 8.7 cells/high-power field [HPF], respectively) compared with VM specimens (9.0 ± 9.8, 1.5 ± 2.4, and 2.5 ± 4.1 cells/HPF, respectively) and normal skin (6.1 ± 8.5, 0.5 ± 1.2, and 1.9 ± 3.4 cells/HPF, respectively). Proliferating IH displayed fewer E2 positive MCs (14.0 6.3 cells/HPF) compared with early (22.3 ± 10.2 cells/HPF, P = 0.023) and late (22.4 ± 6.8 cells/HPF, P = 0.006) involuting specimens. In addition, proliferating IH showed fewer tryptase positive MCs (24.7 ± 10.8 cells/HPF) compared with early involuting specimens (35.7 ± 15.3 cells/HPF, P = 0.043). All IH specimens were ER-a positive and ER-β negative.
Conclusions: E2 and ER-a are expressed on MCs and not on IH endothelial cells. Furthermore, activated MCs may be involved in IH regression.
Keywords: Estradiol; Estrogen receptor; Infantile hemangioma; Mast cells.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Institutional Review Board of the University of Arkansas for Medical Sciences.
Informed consent has obtained from 29 patients.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Munden A, Butschek R, Tom WL, Marshall JS, Poeltler DM, Krohne SE, Alió AB, Ritter M, Friedlander DF, Catanzarite V, Mendoza A, Smith L, Friedlander M, Friedlander SF. Prospective study of infantile haemangiomas: incidence, clinical characteristics and association with placental anomalies. Br J Dermatol. 2014;170:907–913. doi: 10.1111/bjd.12804. - DOI - PMC - PubMed
-
- Mulliken JB, Bischoff J. Pathogenesis of infantile hemangioma. In: Mulliken JB, Burrows PE, Fishman SJ, editors. Vascular anomalies: hemangiomas and malformations. 2. New York: Oxford University Press; 2013. pp. 43–67.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
