

Comparative efficacy of treatment strategies for hepatocellular carcinoma: systematic review and network meta-analysis
- PMID: 30341113
- PMCID: PMC6196801
- DOI: 10.1136/bmjopen-2017-021269
Comparative efficacy of treatment strategies for hepatocellular carcinoma: systematic review and network meta-analysis
Abstract
Objective: Hepatocellular carcinoma (HCC) is the third leading cause of cancer death worldwide. We conducted network meta-regression within a Bayesian framework to compare and rank different treatment strategies for HCC through direct and indirect evidence from international studies.
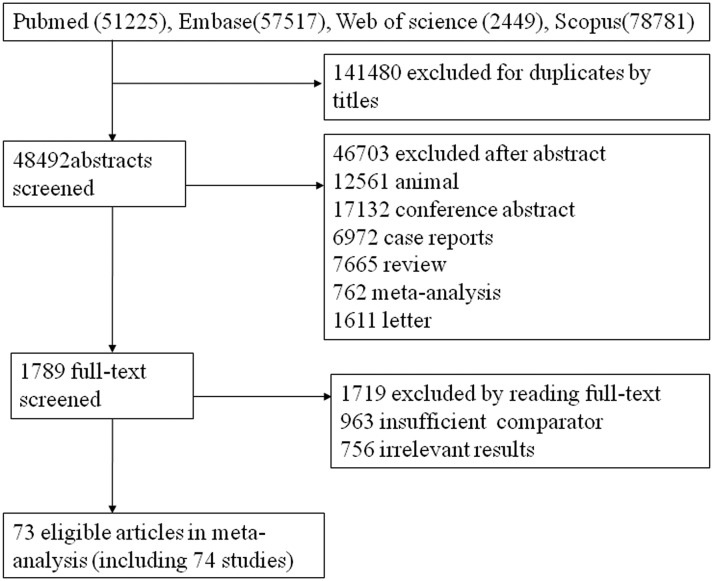
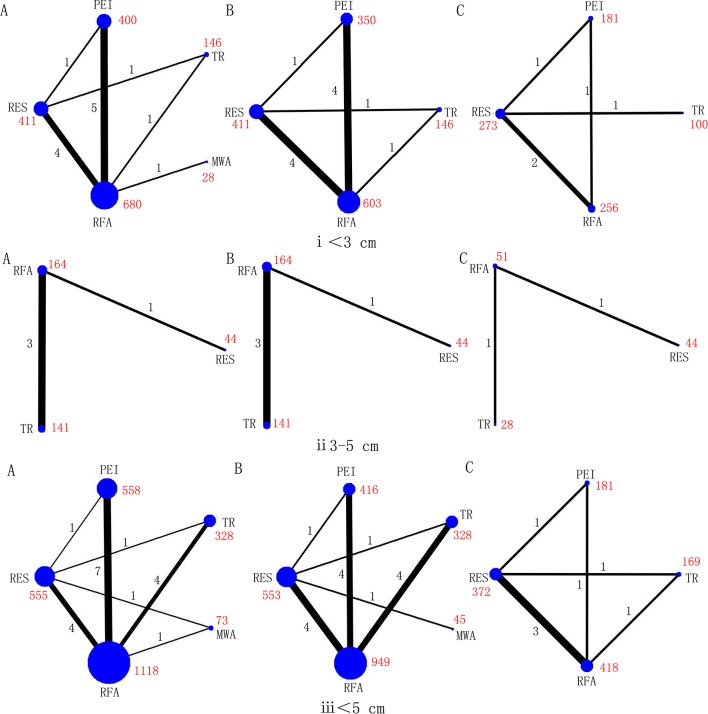
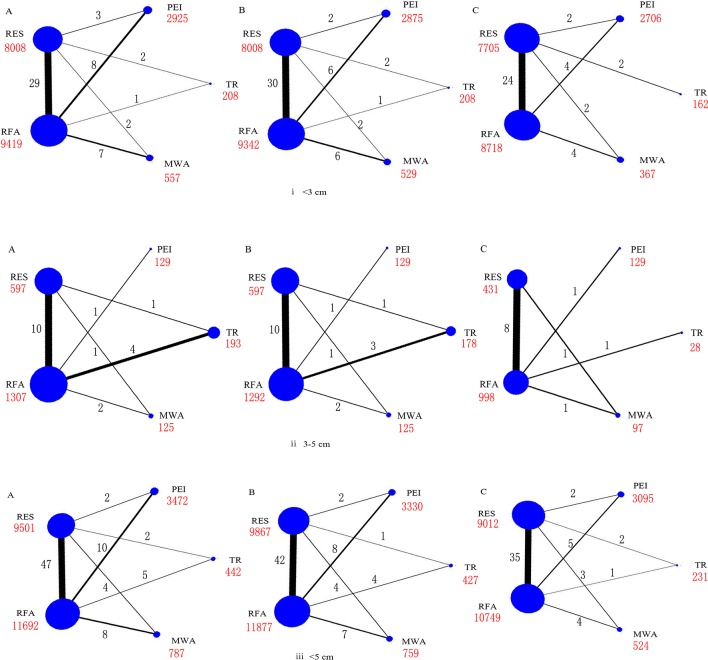
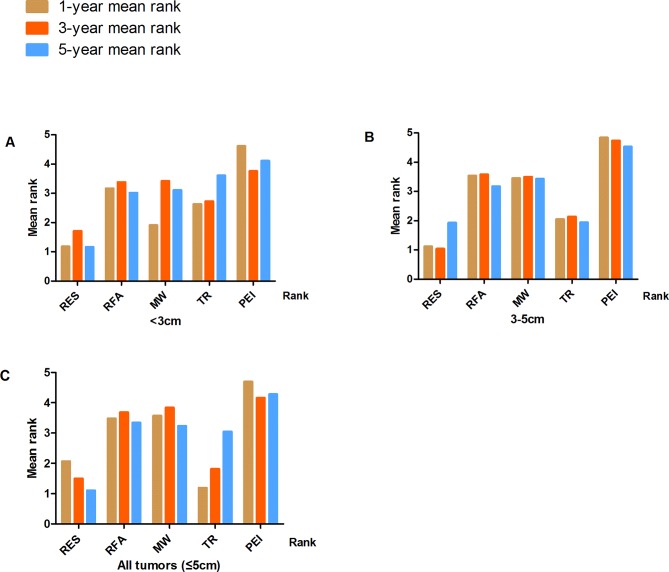
Methods and analyses: We pooled the OR for 1-year, 3-year and 5-year overall survival, based on lesions of size ˂ 3 cm, 3-5 cm and ≤5 cm, using five therapeutic options including resection (RES), radiofrequency ablation (RFA), microwave ablation (MWA), transcatheter arterial chemoembolisation (TACE) plus RFA (TR) and percutaneous ethanol injection (PEI).
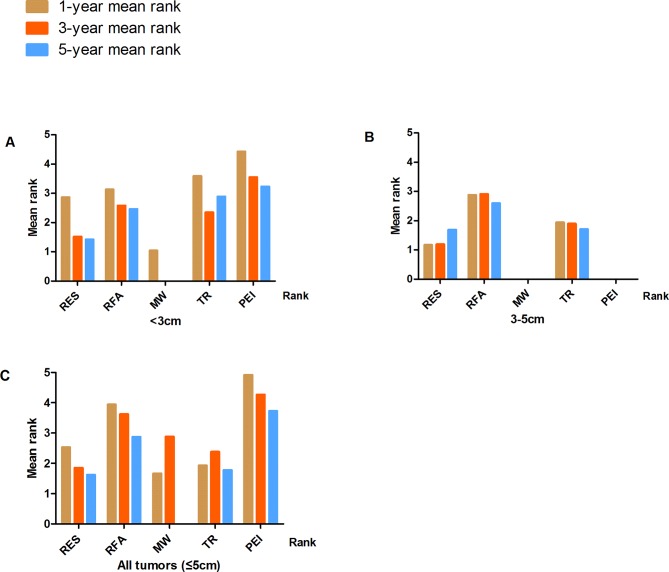
Results: We identified 74 studies, including 26 944 patients. After adjustment for study design, and in the full sample of studies, the treatments were ranked in order of greatest to least benefit as follows for 5 year survival: (1) RES, (2) TR, (3) RFA, (4) MWA and (5) PEI. The ranks were similar for 1- and 3-year survival, with RES and TR being the highest ranking treatments. In both smaller (<3 cm) and larger tumours (3-5 cm), RES and TR were also the two highest ranking treatments. There was little evidence of inconsistency between direct and indirect evidence.
Conclusion: The comparison of different treatment strategies for HCC indicated that RES is associated with longer survival. However, many of the between-treatment comparisons were not statistically significant and, for now, selection of strategies for treatment will depend on patient and disease characteristics. Additionally, much of the evidence was provided by non-randomised studies and knowledge gaps still exist. More head-to-head comparisons between both RES and TR, or other approaches, will be necessary to confirm these findings.
Keywords: hepatocellular carcinoma; microwave ablation; percutaneous ethanol injection; radiofrequency ablation; resection; transcatheter arterial chemoembolization.
© Author(s) (or their employer(s)) 2018. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- GMaCoD C. GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;385:117–71. 10.1016/S0140-6736(14)61682-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous