

Ordinal vs dichotomous analyses of modified Rankin Scale, 5-year outcome, and cost of stroke
- PMID: 30341155
- PMCID: PMC6260198
- DOI: 10.1212/WNL.0000000000006554
Ordinal vs dichotomous analyses of modified Rankin Scale, 5-year outcome, and cost of stroke
Abstract
Objective: To compare how 3 common representations (ordinal vs dichotomized as 0-1/2-6 or 0-2/3-6) of the modified Rankin Scale (mRS)-a commonly used trial outcome measure-relate to long-term outcomes, and quantify trial ineligibility rates based on premorbid mRS.
Methods: In consecutive patients with ischemic stroke in a population-based, prospective, cohort study (Oxford Vascular Study; 2002-2014), we related 3-month mRS to 1-year and 5-year disability and death (logistic regressions), and health/social care costs (generalized linear model), adjusted for age/sex, and compared goodness-of-fit values (C statistic, mean absolute error). We also calculated the proportion of patients in whom premorbid mRS score >1 or >2 would result in exclusion from trials using dichotomous analysis.
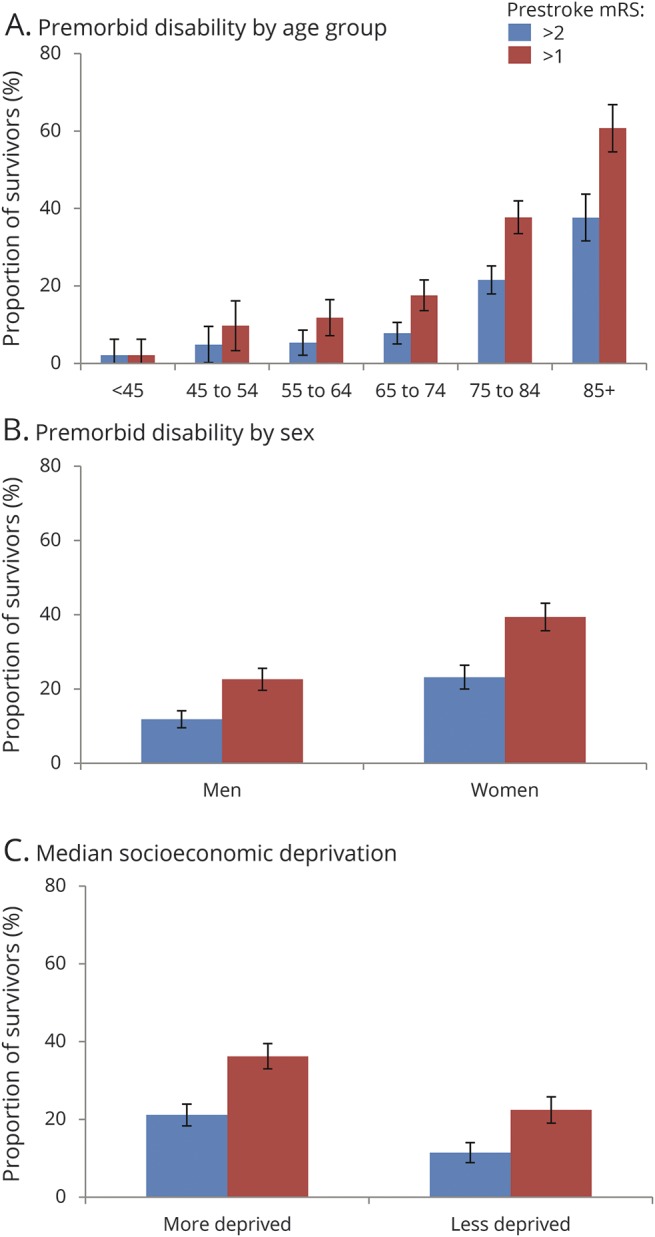
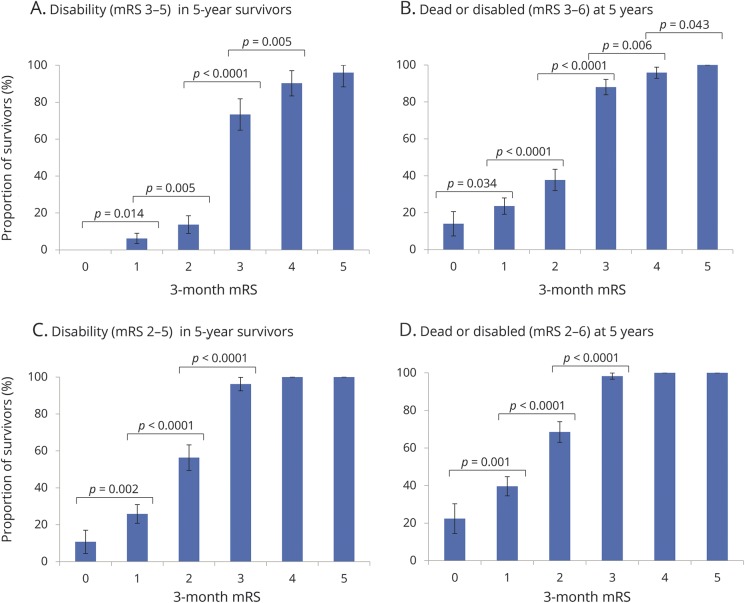
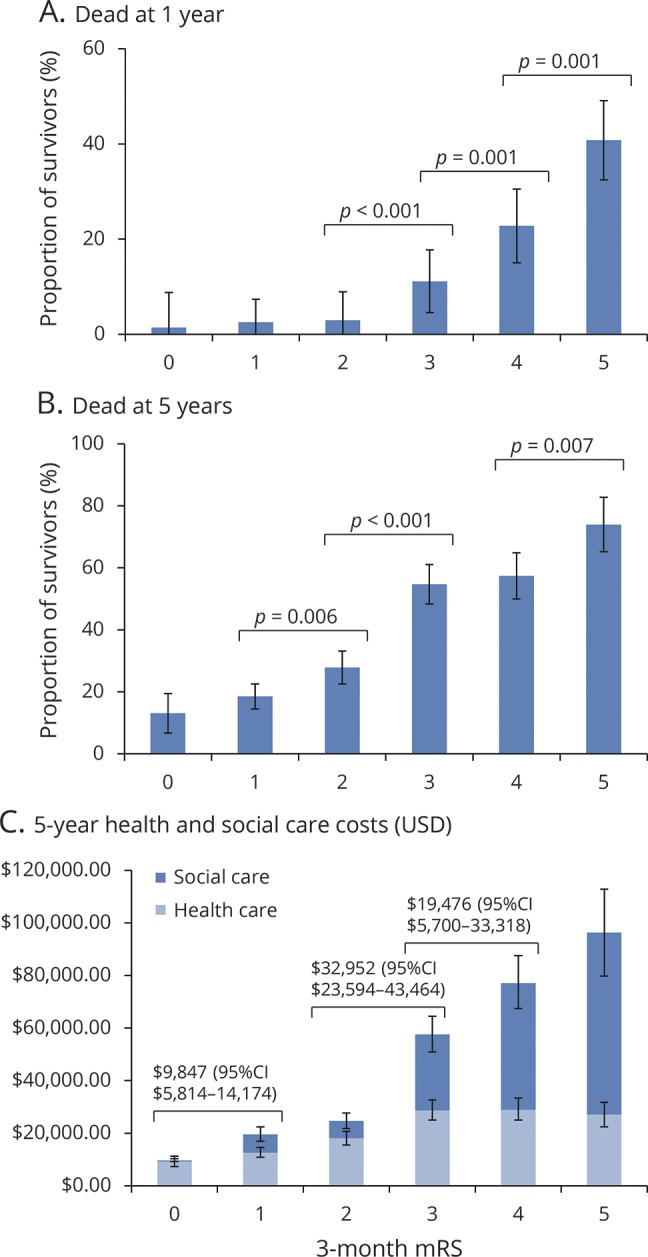
Results: Among 1,607 patients, the ordinal mRS was more strongly related to 5-year mortality than both the 0-1/2-6 and 0-2/3-6 dichotomies (all p < 0.0001). Results were similar for 5-year disability, and 5-year care costs were also best captured by the ordinal model (change in mean absolute error vs age/sex: -$3,059 for ordinal, -$2,805 for 0-2/3-6, -$1,647 for 0-1/2-6). Two hundred forty-four (17.1%) 3-month survivors had premorbid mRS score >2 and 434 (30.5%) had mRS score >1; both proportions increased with female sex, socioeconomic deprivation, and age (all p < 0.0001).
Conclusion: The ordinal form of the 3-month mRS relates better to long-term outcomes and costs in survivors of ischemic stroke than either dichotomy. This finding favors using ordinal approaches in trials analyzing the mRS. Exclusion of patients with higher premorbid disability by use of dichotomous primary outcomes will also result in unrepresentative samples.
Copyright © 2018 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Which version of the modified Rankin Scale should we use for stroke trials? Lump or split?Neurology. 2018 Nov 20;91(21):947-948. doi: 10.1212/WNL.0000000000006533. Epub 2018 Oct 19. Neurology. 2018. PMID: 30341157 No abstract available.
-
Reader response: Ordinal vs dichotomous analyses of modified Rankin Scale, 5-year outcome, and cost of stroke.Neurology. 2019 Oct 15;93(16):724-725. doi: 10.1212/WNL.0000000000008327. Neurology. 2019. PMID: 31611319 No abstract available.
-
Author response: Ordinal vs dichotomous analyses of modified Rankin Scale, 5-year outcome, and cost of stroke.Neurology. 2019 Oct 15;93(16):725. doi: 10.1212/WNL.0000000000008328. Neurology. 2019. PMID: 31611320 No abstract available.
Similar articles
-
Long-Term Consequences of Worsened Poststroke Status in Patients With Premorbid Disability.Stroke. 2018 Oct;49(10):2430-2436. doi: 10.1161/STROKEAHA.118.022416. Stroke. 2018. PMID: 30355105 Free PMC article.
-
Weights for ordinal analyses of the modified Rankin Scale in stroke trials: A population-based cohort study.EClinicalMedicine. 2020 Jun 15;23:100415. doi: 10.1016/j.eclinm.2020.100415. eCollection 2020 Jun. EClinicalMedicine. 2020. PMID: 32577611 Free PMC article.
-
Time Course of Evolution of Disability and Cause-Specific Mortality After Ischemic Stroke: Implications for Trial Design.J Am Heart Assoc. 2017 Jun 11;6(6):e005788. doi: 10.1161/JAHA.117.005788. J Am Heart Assoc. 2017. PMID: 28603141 Free PMC article.
-
Health Utility Weighting of the Modified Rankin Scale: A Systematic Review and Meta-analysis.JAMA Netw Open. 2020 Apr 1;3(4):e203767. doi: 10.1001/jamanetworkopen.2020.3767. JAMA Netw Open. 2020. PMID: 32347948 Free PMC article.
-
Standardized Nomenclature for Modified Rankin Scale Global Disability Outcomes: Consensus Recommendations From Stroke Therapy Academic Industry Roundtable XI.Stroke. 2021 Aug;52(9):3054-3062. doi: 10.1161/STROKEAHA.121.034480. Epub 2021 Jul 29. Stroke. 2021. PMID: 34320814
Cited by
-
Reduced Impact of Endovascular Thrombectomy on Disability in Real-World Practice, Relative to Randomized Controlled Trial Evidence in Australia.Front Neurol. 2020 Dec 8;11:593238. doi: 10.3389/fneur.2020.593238. eCollection 2020. Front Neurol. 2020. PMID: 33363508 Free PMC article.
-
Disabling stroke in persons already with a disability: Ethical dimensions and directives.Neurology. 2020 Feb 18;94(7):306-310. doi: 10.1212/WNL.0000000000008964. Epub 2020 Jan 22. Neurology. 2020. PMID: 31969466 Free PMC article.
-
Very Early MoCA Can Predict Functional Dependence at 3 Months After Stroke: A Longitudinal, Cohort Study.Front Neurol. 2019 Oct 11;10:1051. doi: 10.3389/fneur.2019.01051. eCollection 2019. Front Neurol. 2019. PMID: 31681142 Free PMC article.
-
Seeing the good in the bad: actual clinical outcome of thrombectomy stroke patients with formally unfavorable outcome.Neuroradiology. 2022 Jul;64(7):1429-1436. doi: 10.1007/s00234-022-02920-1. Epub 2022 Mar 8. Neuroradiology. 2022. PMID: 35257206 Free PMC article.
-
Arachnoid granulations may be protective against the development of shunt dependent chronic hydrocephalus after aneurysm subarachnoid hemorrhage*.Neuroradiol J. 2023 Apr;36(2):189-193. doi: 10.1177/19714009221122249. Epub 2022 Aug 21. Neuroradiol J. 2023. PMID: 35993411 Free PMC article.
References
-
- Saver JL, Goyal M, van der Lugt A, et al. . Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. JAMA 2016;316:1279–1288. - PubMed
-
- Anderson CS, Robinson T, Lindley RI, et al. . Low-dose versus standard-dose intravenous alteplase in acute ischemic stroke. New Engl J Med 2016;374:2313–2323. - PubMed
-
- Thomalla G, Fiebach JB, Ostergaard L, et al. . A multicenter, randomized, double-blind, placebo-controlled trial to test efficacy and safety of magnetic resonance imaging-based thrombolysis in wake-up stroke (WAKE-UP). Int J Stroke 2014;9:829–836. - PubMed
-
- Bath PM, Lees KR, Schellinger PD, et al. . Statistical analysis of the primary outcome in acute stroke trials. Stroke 2012;43:1171–1178. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical