

Cortico-efferent tract involvement in primary lateral sclerosis and amyotrophic lateral sclerosis: A two-centre tract of interest-based DTI analysis
- PMID: 30343251
- PMCID: PMC6198122
- DOI: 10.1016/j.nicl.2018.10.005
Cortico-efferent tract involvement in primary lateral sclerosis and amyotrophic lateral sclerosis: A two-centre tract of interest-based DTI analysis
Abstract
Background: After the demonstration of a corticoefferent propagation pattern in amyotrophic lateral sclerosis (ALS) by neuropathological studies, this concept has been used for in vivo staging of individual patients by diffusion tensor imaging (DTI) techniques, both in `classical` ALS and in restricted phenotypes such as primary lateral sclerosis (PLS).
Objective: The study was designed to investigate that microstructural changes according to the neuropathologically defined ALS alteration pattern in PLS patients could be confirmed to be identical to ´classical´ ALS patients. The novelty in this approach is that the results were independent of the subject samples and the data acquisition parameters (as was validated in two samples from two different centres). That way, reproducibility across (international) centres in addition to harmonisation/standardisation of data analysis has been addressed, for the possible use of MRI-based staging to stratify patients in clinical trials.
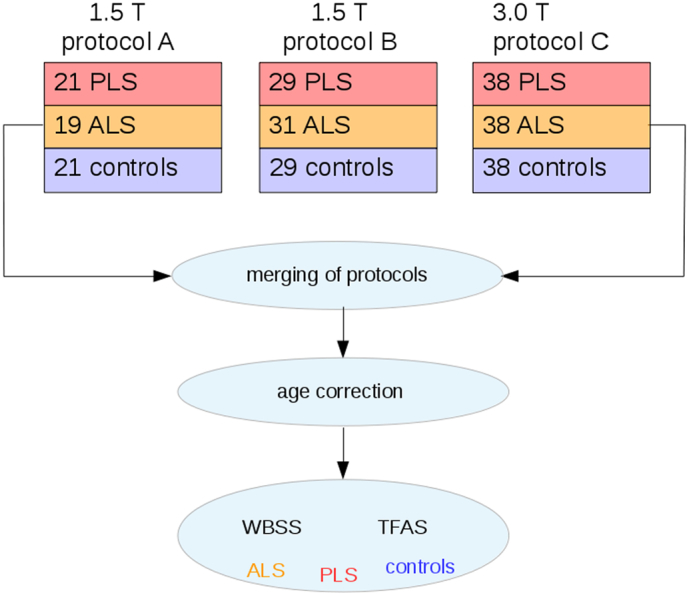
Methods: Tractwise analysis of fractional anisotropy (FA) maps according to the ALS-staging pattern was applied to DTI data (pooled from two ALS centres) of 88 PLS patients and 88 ALS patients with a 'classical' phenotype in comparison to 88 matched controls in order to identify white matter integrity alterations.
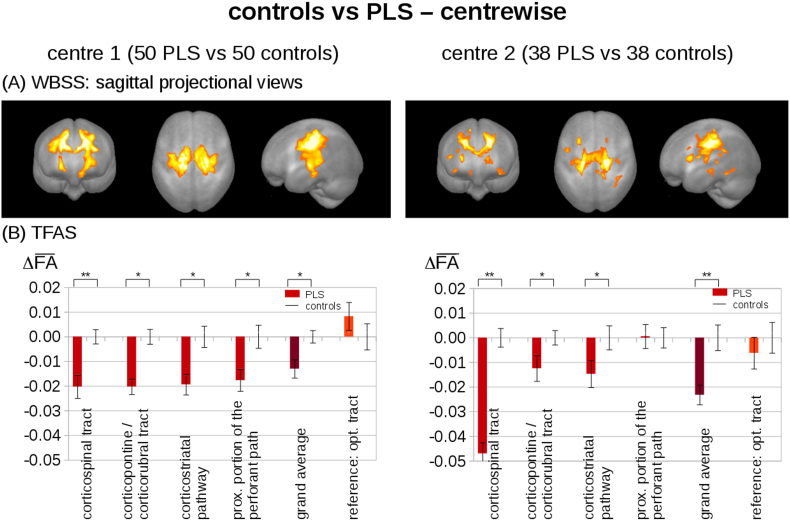
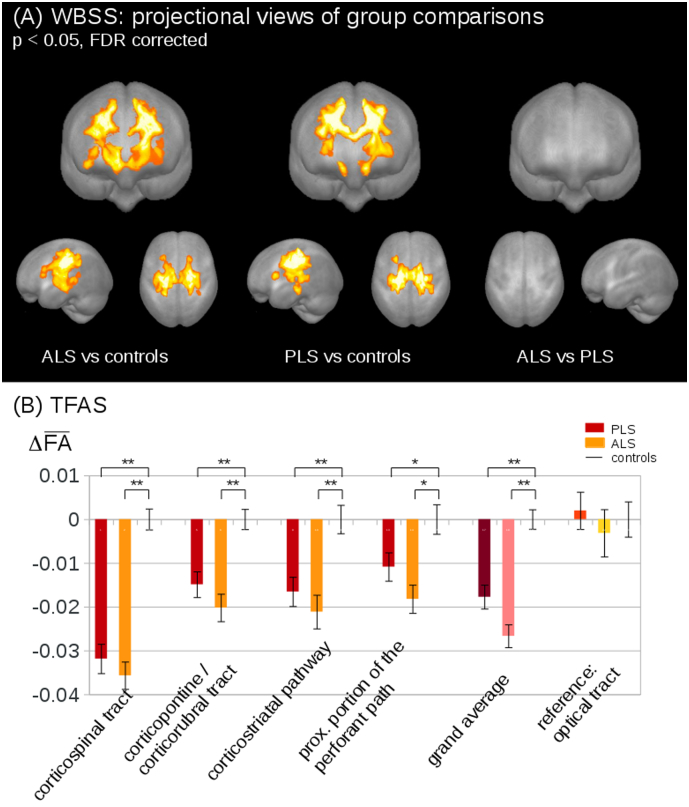
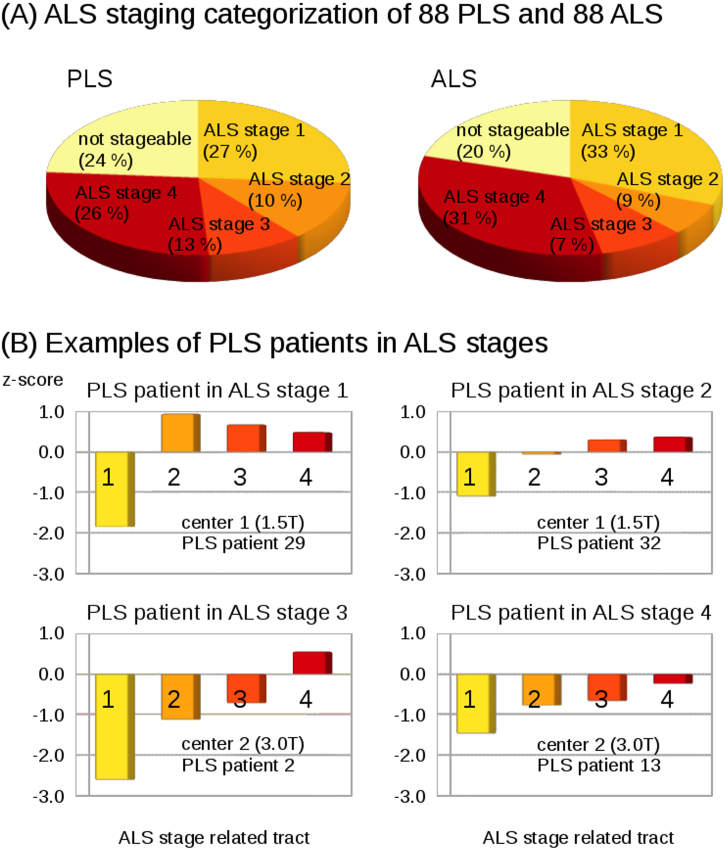
Results: In the tract-specific analysis, alterations were identical for PLS and ALS in the tract systems corresponding to the ALS staging pattern, independent of the subject samples and the data acquisition parameters. The individual categorisation into ALS stages did not differ between PLS and ALS patients.
Conclusions: This DTI study in a two-centre setting demonstrated that the neuropathological stages can be mapped in vivo in PLS with high reproducibility and that PLS-associated cerebral propagation, although showing the same corticofugal patterns as ALS, might have a different time course of neuropathology, in analogy to its much slower clinical progression rates.
Keywords: Amyotrophic lateral sclerosis; Diffusion tensor imaging; Magnetic resonance imaging; Motor neuron disease; Primary lateral sclerosis.
Copyright © 2018 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The same cortico-efferent tract involvement in progressive bulbar palsy and in 'classical' ALS: A tract of interest-based MRI study.Neuroimage Clin. 2019;24:101979. doi: 10.1016/j.nicl.2019.101979. Epub 2019 Aug 9. Neuroimage Clin. 2019. PMID: 31421506 Free PMC article.
-
Identical patterns of cortico-efferent tract involvement in primary lateral sclerosis and amyotrophic lateral sclerosis: A tract of interest-based MRI study.Neuroimage Clin. 2018 Mar 15;18:762-769. doi: 10.1016/j.nicl.2018.03.018. eCollection 2018. Neuroimage Clin. 2018. PMID: 29785360 Free PMC article.
-
Fast progressive lower motor neuron disease is an ALS variant: A two-centre tract of interest-based MRI data analysis.Neuroimage Clin. 2017 Oct 14;17:145-152. doi: 10.1016/j.nicl.2017.10.008. eCollection 2018. Neuroimage Clin. 2017. PMID: 29071208 Free PMC article.
-
Diffusion Tensor Imaging in Amyotrophic Lateral Sclerosis: Machine Learning for Biomarker Development.Int J Mol Sci. 2023 Jan 18;24(3):1911. doi: 10.3390/ijms24031911. Int J Mol Sci. 2023. PMID: 36768231 Free PMC article. Review.
-
Amyotrophic lateral sclerosis and primary lateral sclerosis: The role of diffusion tensor imaging and other advanced MR-based techniques as objective upper motor neuron markers.Ann N Y Acad Sci. 2005 Dec;1064:61-77. doi: 10.1196/annals.1340.013. Ann N Y Acad Sci. 2005. PMID: 16394148 Review.
Cited by
-
Feature selection from magnetic resonance imaging data in ALS: a systematic review.Ther Adv Chronic Dis. 2021 Oct 13;12:20406223211051002. doi: 10.1177/20406223211051002. eCollection 2021. Ther Adv Chronic Dis. 2021. PMID: 34729157 Free PMC article. Review.
-
Extra-motor cerebral changes and manifestations in primary lateral sclerosis.Brain Imaging Behav. 2021 Oct;15(5):2283-2296. doi: 10.1007/s11682-020-00421-4. Epub 2021 Jan 7. Brain Imaging Behav. 2021. PMID: 33409820
-
The same cortico-efferent tract involvement in progressive bulbar palsy and in 'classical' ALS: A tract of interest-based MRI study.Neuroimage Clin. 2019;24:101979. doi: 10.1016/j.nicl.2019.101979. Epub 2019 Aug 9. Neuroimage Clin. 2019. PMID: 31421506 Free PMC article.
-
Involvement of cortico-efferent tracts in flail arm syndrome: a tract-of-interest-based DTI study.J Neurol. 2022 May;269(5):2619-2626. doi: 10.1007/s00415-021-10854-6. Epub 2021 Oct 21. J Neurol. 2022. PMID: 34676447 Free PMC article.
-
The imaging signature of C9orf72 hexanucleotide repeat expansions: implications for clinical trials and therapy development.Brain Imaging Behav. 2021 Oct;15(5):2693-2719. doi: 10.1007/s11682-020-00429-w. Epub 2021 Jan 5. Brain Imaging Behav. 2021. PMID: 33398779
References
-
- Agosta F., Al-Chalabi A., Filippi M. The El Escorial criteria: strengths and weaknesses. Amyotroph. Lateral Scler. Frontotemporal Degener. 2015;16:1–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
