

Impact of a multifaceted prevention program on ventilator-associated pneumonia including selective oropharyngeal decontamination
- PMID: 30343312
- PMCID: PMC6244525
- DOI: 10.1007/s00134-018-5227-4
Impact of a multifaceted prevention program on ventilator-associated pneumonia including selective oropharyngeal decontamination
Abstract
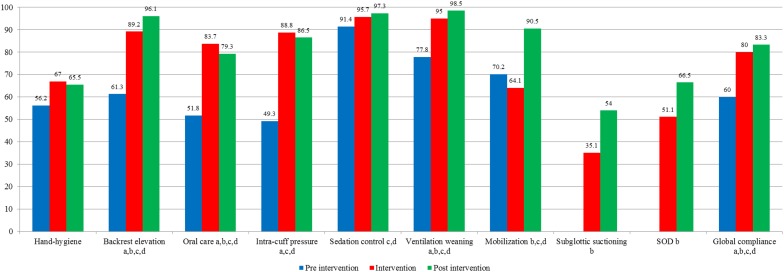
Purpose: We describe the impact of a multifaceted program for decreasing ventilator-associated pneumonia (VAP) after implementing nine preventive measures, including selective oropharyngeal decontamination (SOD).
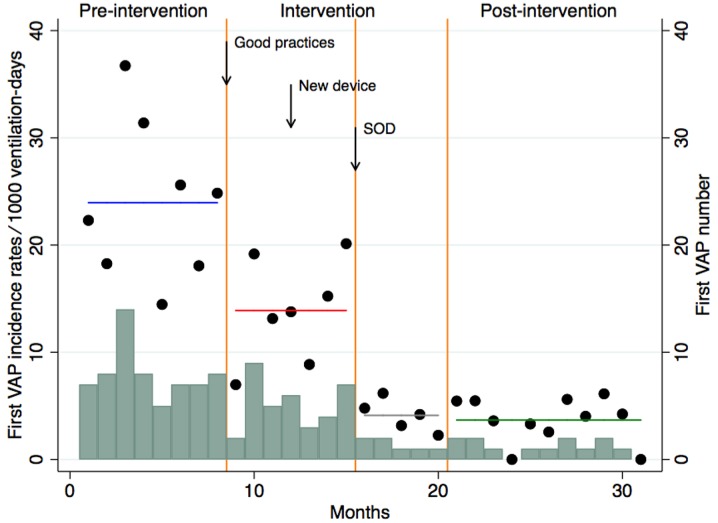
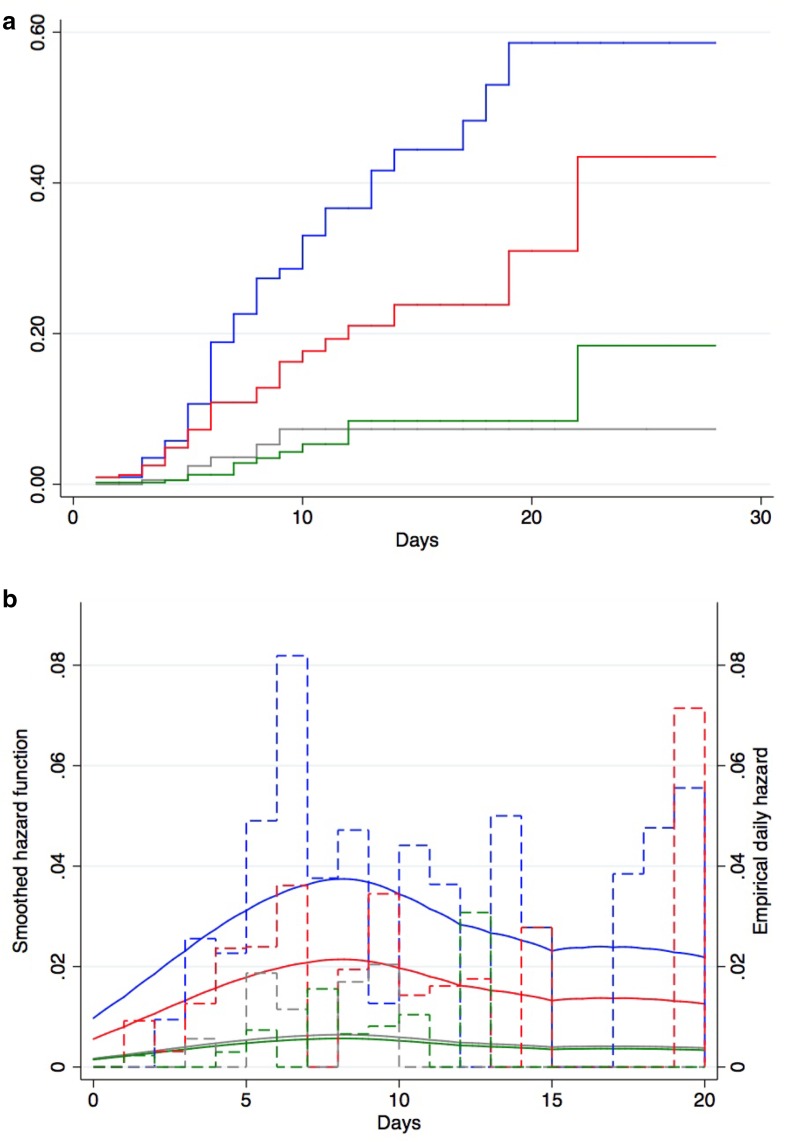
Methods: We compared VAP rates during an 8-month pre-intervention period, a 12-month intervention period, and an 11-month post-intervention period in a cohort of patients who received mechanical ventilation (MV) for > 48 h. The primary objective was to assess the effect on first VAP occurrence, using a Cox cause-specific proportional hazards model. Secondary objectives included the impact on emergence of antimicrobial resistance, antibiotic consumption, duration of MV, and ICU mortality.
Results: Pre-intervention, intervention and post-intervention VAP rates were 24.0, 11.0 and 3.9 VAP episodes per 1000 ventilation-days, respectively. VAP rates decreased by 56% [hazard ratio (HR) 0.44, 95% CI 0.29-0.65; P < 0.001] in the intervention and by 85% (HR 0.15, 95% CI 0.08-0.27; P < 0.001) in the post-intervention periods. During the intervention period, VAP rates decreased by 42% (HR 0.58, 95% CI 0.38-0.87; P < 0.001) after implementation of eight preventive measures without SOD, and by 70% after adding SOD (HR 0.30, 95% CI 0.13-0.72; P < 0.001) compared to the pre-intervention period. The incidence density of intrinsically resistant bacteria (to colistin or tobramycin) did not increase. We documented a significant reduction of days of therapy per 1000 patient-days of broad-spectrum antibiotic used to treat lower respiratory tract infection (P < 0.028), median duration of MV (from 7.1 to 6.4 days; P < 0.003) and ICU mortality (from 16.2 to 13.5%; P < 0.049) for patients ventilated > 48 h between the pre- and post-intervention periods.
Conclusions: Our preventive program produced a sustained decrease in VAP incidence. SOD provides an additive value.
Keywords: Intensive care unit; Multimodal strategy; Selective oropharyngeal decontamination; Ventilator-associated pneumonia.
Conflict of interest statement
Conflicts of interest
SH reports having received a peer-reviewed research grant funded by Pfizer; he is also a temporary member of the advisory boards of DNA Electronics, Bayer and Novartis. All other authors: none to declare.
Research involving human participants
As a quality improvement project, ethics committee approval was not required.
Figures
Comment in
-
Beat around the bush for VA-LRTI.Intensive Care Med. 2018 Nov;44(11):1961-1963. doi: 10.1007/s00134-018-5281-y. Epub 2018 Oct 21. Intensive Care Med. 2018. PMID: 30343316 No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
