

Evolution in Management of Tibial Pilon Fractures
- PMID: 30343399
- PMCID: PMC6220009
- DOI: 10.1007/s12178-018-9519-7
Evolution in Management of Tibial Pilon Fractures
Abstract
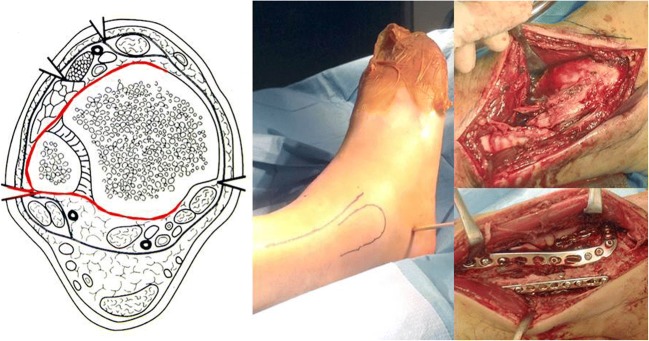
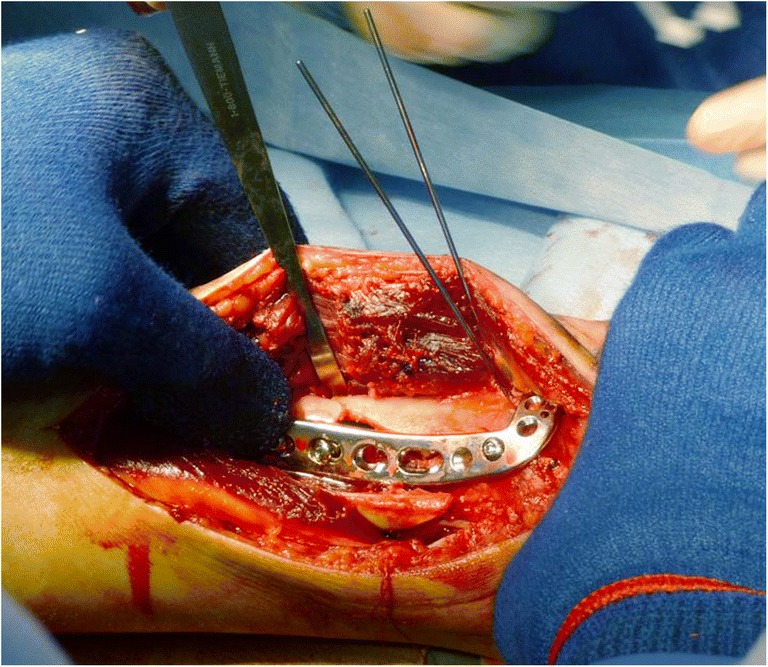
Purpose of review: Tibial plafond, or pilon, fractures can be some of the most difficult fractures to manage. As they are often associated with high-energy trauma, both the soft tissue involvement and the comminuted fracture pattern pose challenges to fixation. Furthermore, the complex anatomy and trauma to the cartilage at the time of injury predispose pilon fractures to poor functional outcomes and high rates of posttraumatic arthritis. This review will discuss the recent developments in the treatment of tibial pilon fractures.
Recent findings: Historically, surgical management of pilon fractures has been associated with high rates of complications, including wound complications, infections, nonunions, and even the need for amputation. In response, staged protocols were created. However, recent studies have called this into question, demonstrating low wound complications with early definitive fixation. Additional studies are evaluating adjuvants to minimize wound complications, including the use of vancomycin powder and oxygen supplementation, while another study challenges the 7-cm myth regarding the distance needed between skin incisions. Additional research has been focused on alternative methods of managing these complex, and sometimes non-reconstructable, injuries with the use of external fixation, minimally invasive internal fixation, and primary arthrodesis. Tibial pilon fractures remain difficult to treat for even the most skilled orthopedic trauma surgeons. With improvements in surgical techniques and implants, complication rates have declined and outcomes have improved; however, the overall prognosis for these injuries often remains poor.
Keywords: Distal tibia fracture; Intra-articular fracture; Pilon fracture; Plafond fracture.
Conflict of interest statement
Conflict of Interest
All authors declare no conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures




References
-
- Mauffrey C, Vasario G, Battiston B, Lewis C, Beazley J, Seligson D. Tibial pilon fractures: a review of incidence, diagnosis, treatment, and complications. Acta Orthop Belg. 2011;77(4):432–440. - PubMed
-
- •• White TO, Guy P, Cooke CJ, et al. The results of early primary open reduction and internal fixation for treatment of OTA 43.C-type tibial pilon fractures: a cohort study. J Orthop Trauma. 2010;24(12):757–63. A study of 95 patients underwent early definitive fixation of AO/OTA type 43C pilon fractures. Ninety-eight percent of patients were treated within 48 h of presentation. Wound complications were noted in 19% of open fractures and 2.7% of closed fractures. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials
