

Diagnosis of incarcerated intramesosigmoid hernia aided by multiplanar reconstruction images of multidetector computed tomography: a case report
- PMID: 30343419
- PMCID: PMC6195874
- DOI: 10.1186/s40792-018-0535-z
Diagnosis of incarcerated intramesosigmoid hernia aided by multiplanar reconstruction images of multidetector computed tomography: a case report
Abstract
Background: Internal hernia is a rare cause of intestinal obstruction, and sigmoid mesocolon hernia is an extremely rare form of this condition. Among sigmoid mesocolon hernias, intramesosigmoid hernia is the least frequent subtype. We described a case of intramesosigmoid hernia through the orifice on the right leaf of the mesosigmoid with an incarcerated ileum of 6 cm in length without strangulation. This case was diagnosed by multidetector computed tomography with multiplanar reconstruction images and treated without resection of the small intestine in a 52-year-old man with characteristic diagnostic images.
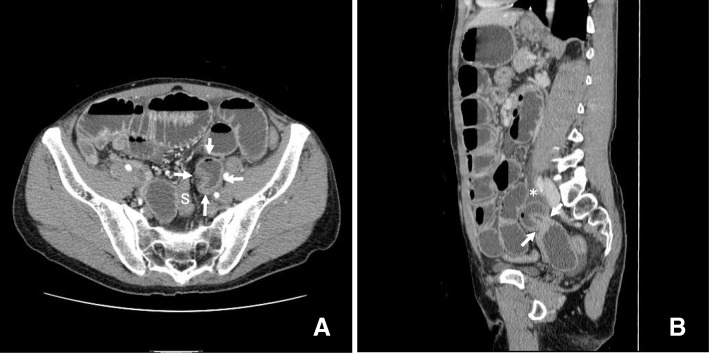
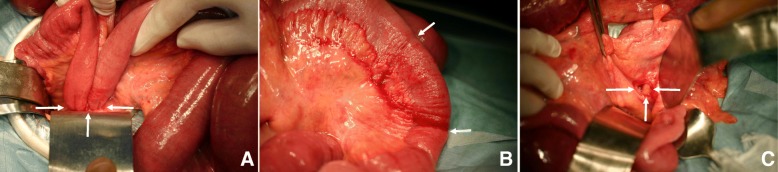
Case presentation: A 52-year-old man suffering periumbilical cramping pain with sudden onset that had persisted for 1 week without recovery was referred to Fukui Katsuyama General Hospital. Multidetector computed tomography revealed small bowel obstruction, and an incarcerated short intestinal loop was revealed by sagittal slices of the multiplanar reconstruction images of the routine study of the left side of the pelvic space. Sagittal multiplanar reconstruction images also showed narrow belt-shaped fluid retention contacting the tip of the incarcerated short loop toward the cranial direction localized in the mesosigmoid. These findings indicated that the fluid and the herniated small bowel were wrapped together in the mesosigmoid, which was characteristic of intramesosigmoid hernia. The patient underwent laparotomy operation 2 days after admission. The ileum, which was approximately 75 cm proximal to the ileocecal junction and herniated into the mesosigmoid through the right leaf, was released without resection. The orifice located in the central part of the right leaf was oval shaped and measured less than 2 cm in diameter. The left leaf of the mesosigmoid was intact. The orifice of the right lobe was closed by suture. The patient showed an uneventful recovery.
Conclusion: We report an extremely rare case of incarcerated intramesosigmoid hernia that was diagnosed by multidetector computed tomography with multiplanar reconstruction images. The finding of narrow belt-shaped fluid retention contacting the tip of the incarcerated short intestinal loop is characteristic of intramesosigmoid hernia and will be useful for conclusively differentiating this disease from transmesosigmoid hernia. Although intramesosigmoid hernia is a rare cause of internal hernia, multidetector computed tomography and multiplanar reconstruction images can provide the characteristic findings and proved useful for the precise preoperative diagnosis and treatment of intramesosigmoid hernia.
Keywords: Intramesosigmoid hernia; MDCT; MPR; Sigmoid mesocolon hernia.
Conflict of interest statement
Ethics approval and consent to participate
All procedures used in this research were approved by the Ethical Committee of the Japan Community Health Care Organization.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this Journal.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Laparoscopic treatment of small bowel strangulation caused by an intramesosigmoid hernia and review of literature.BMJ Case Rep. 2020 Apr 29;13(4):e233627. doi: 10.1136/bcr-2019-233627. BMJ Case Rep. 2020. PMID: 32354762 Free PMC article. Review.
-
A case of an intramesosigmoid hernia.J Nippon Med Sch. 2009 Feb;76(1):13-8. doi: 10.1272/jnms.76.13. J Nippon Med Sch. 2009. PMID: 19305105
-
Strangulation of the small intestine caused by an intra-mesosigmoid hernia: a case report.Surg Case Rep. 2017 Dec 21;3(1):129. doi: 10.1186/s40792-017-0406-z. Surg Case Rep. 2017. PMID: 29270809 Free PMC article.
-
Usefulness of Oblique Multiplanar Images on Multi-Detector Computed Tomography for Diagnosing Intersigmoid Hernia.Visc Med. 2016 Dec;32(6):437-440. doi: 10.1159/000450633. Epub 2016 Nov 22. Visc Med. 2016. PMID: 28229081 Free PMC article.
-
Intersigmoid hernia: Report of a case.Surg Today. 2010;40(2):171-5. doi: 10.1007/s00595-009-4010-0. Epub 2010 Jan 28. Surg Today. 2010. PMID: 20107960 Review.
Cited by
-
Laparoscopic treatment of small bowel strangulation caused by an intramesosigmoid hernia and review of literature.BMJ Case Rep. 2020 Apr 29;13(4):e233627. doi: 10.1136/bcr-2019-233627. BMJ Case Rep. 2020. PMID: 32354762 Free PMC article. Review.
-
Congenital Dual Internal Hernias Causing Small Bowel Obstruction in a Man with no Prior Surgical History: A Report of a Very Rare Case.Am J Case Rep. 2021 Jul 13;22:e932132. doi: 10.12659/AJCR.932132. Am J Case Rep. 2021. PMID: 34255765 Free PMC article.
References
LinkOut - more resources
Full Text Sources
