

Langerhans' Cell Histiocytosis Masquerading as Metastatic Papillary Thyroid Cancer on F-18 FDG PET/CT: Diagnostic Dilemma Solved by PET/CT-Guided Biopsy
- PMID: 30344790
- PMCID: PMC6177344
- DOI: 10.1007/s13139-018-0536-7
Langerhans' Cell Histiocytosis Masquerading as Metastatic Papillary Thyroid Cancer on F-18 FDG PET/CT: Diagnostic Dilemma Solved by PET/CT-Guided Biopsy
Abstract
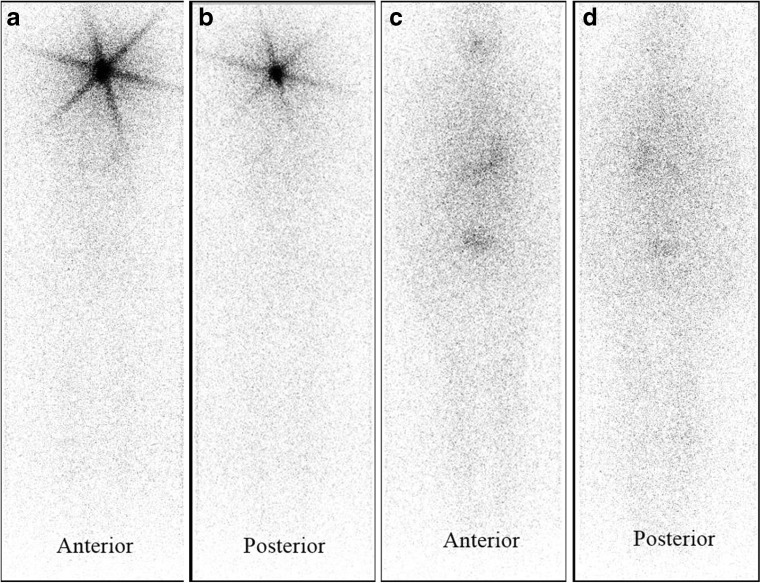
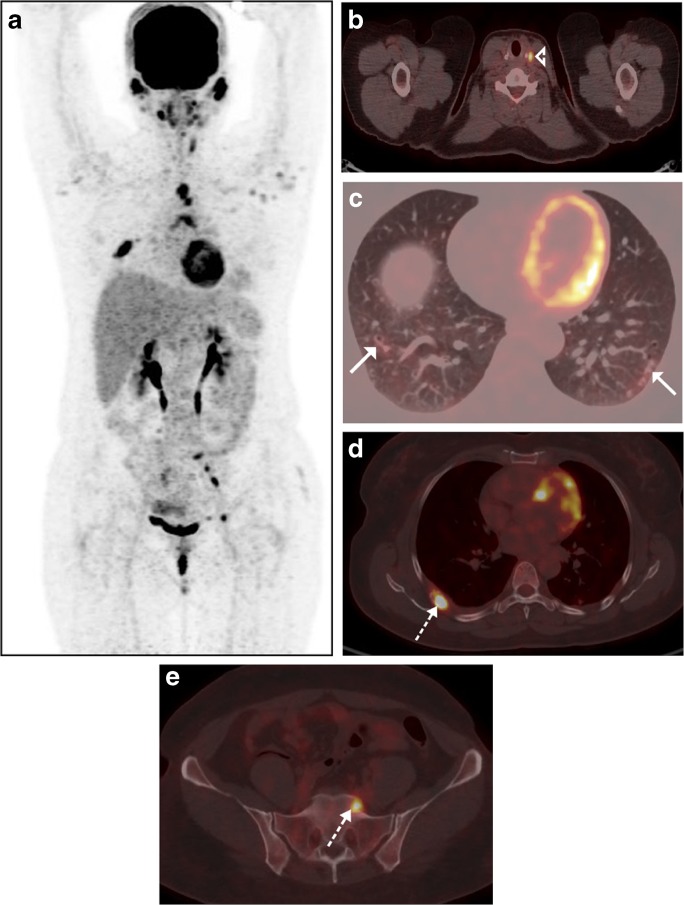
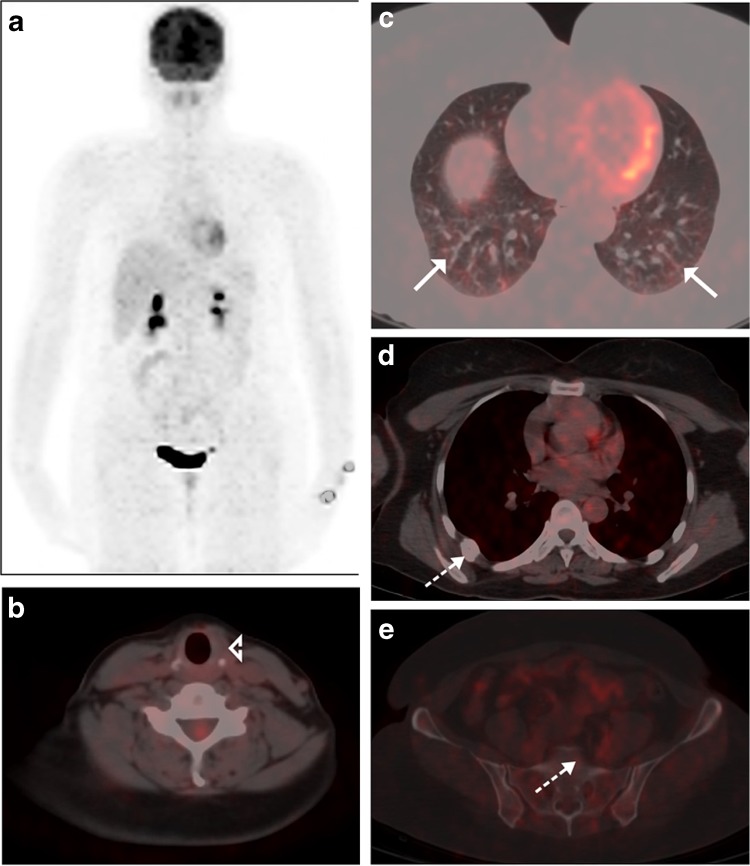
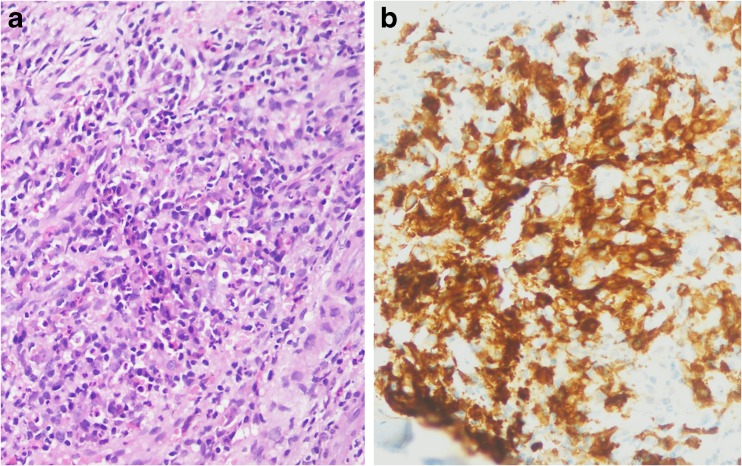
We present a case of papillary thyroid cancer (post-thyroidectomy status) on regular treatment with suppressive Levothyroxine therapy. On follow-up at 6 months after radioactive iodine ablation for remnant thyroid tissue, her thyroglobulin, and anti-thyroglobulin levels were 0.06 ng/ml and 670 IU/ml, respectively. Low-dose whole-body I-131 scan was negative. To look for the cause of isolated increased anti-thyroglobulin level, a whole-body 18F-FDG PET/CT was done which revealed multiple FDG-avid lytic skeletal lesions suggestive of metastases. For confirmation of diagnosis, 18F-FDG PET/CT-guided metabolic biopsy was done, which revealed Langerhans' cell histiocytosis on histopathological examination.
Keywords: 18F-FDG PET/CT; Anti-thyroglobulin level; Langerhans’ cell histiocytosis; PET/CT-guided biopsy; Papillary thyroid cancer.
Conflict of interest statement
Dharmender Malik, Rajender Kumar Basher, Bhagwant Rai Mittal, Gaurav Parkash, Amanjit Bal, and Anish Bhattacharya declare that they have no conflict of interest.All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.The institutional review board of our institute approved this retrospective study, and the requirement to obtain informed consent was waived.
Figures
References
-
- Qiu ZL, Wei WJ, Shen CT, Song HJ, Zhang XY, Sun ZK, et al. Diagnostic performance of 18F-FDG PET/CT in papillary thyroid carcinoma with negative 131I-WBS at first post-ablation, negative Tg and progressively increased TgAb level. Sci Rep. 2017;7:2849. doi: 10.1038/s41598-017-03001-7. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources