

Transcervical videomediastino-thoracoscopy
- PMID: 30345101
- PMCID: PMC6178289
- DOI: 10.21037/jtd.2018.03.132
Transcervical videomediastino-thoracoscopy
Abstract
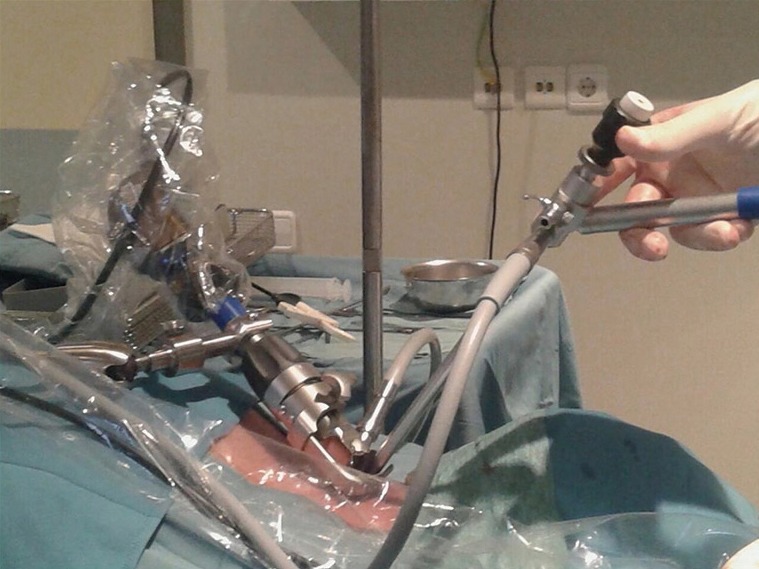
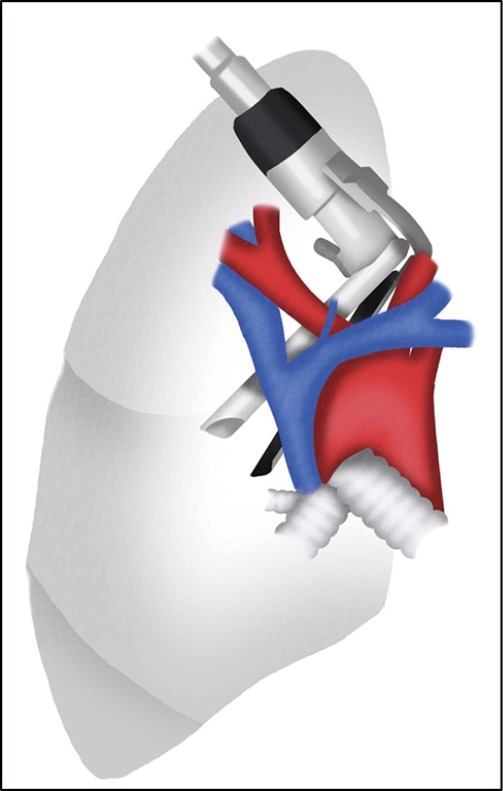
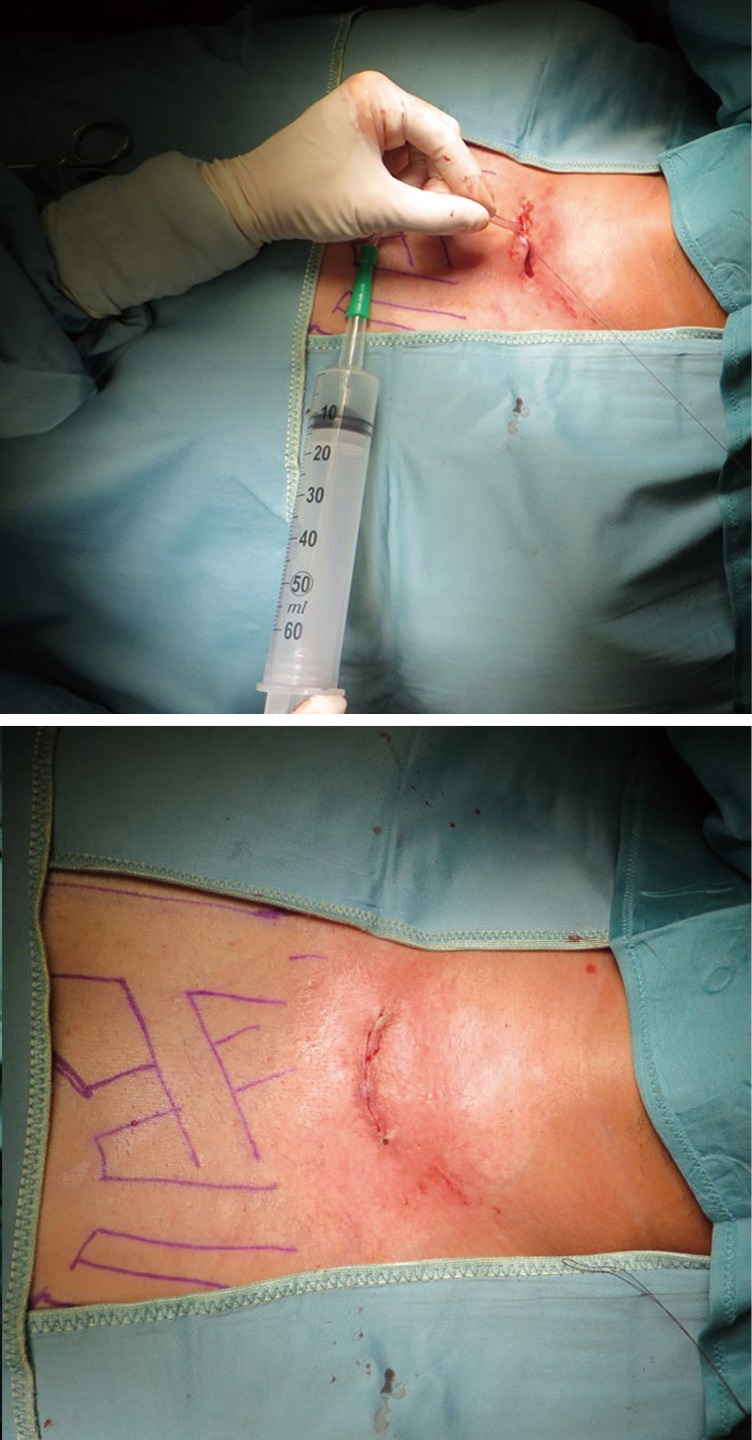
Although technical advances in non-invasive and minimally invasive approaches to lung and pleural cancer diagnosis and staging have become more widely available and accurate, surgical techniques remain the gold standard in assessing the extent of loco-regional involvement. Precise surgical staging of lung or pleural tumours is pivotal in the selection of surgical candidates and for predicting survival. In some patients, both mediastinal and pleural exploration may be needed for many different reasons. Transcervical videomediastino-thoracoscopy (VMT) combines simultaneously the exploration of both the mediastinum and the pleural cavities through a single cervical incision, allowing for biopsies or sampling of the mediastinal lymph nodes, lymphadenectomy and pleuropulmonary assessment (mainly pleural effusions, tumour involvement of the visceral and parietal pleura and pulmonary nodules). Thoracic surgeons should be aware of this combined surgical approach and completely familiar with classical indications and technical details of the transcervical approach to the mediastinum and thoracoscopic exploration of the pleural cavities.
Keywords: Staging; lung cancer; thoracoscopy; videomediastinoscopy.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures









References
-
- Rami-Porta R, Call S, Serra-Mitjans M. Mediastinoscopy. In: Zieliński M, Rami-Porta R. editors. The Transcervical Approach in Thoracic Surgery. Heidelberg: Springer-Verlag, 2014:9-27.
-
- Witte B, Wolf M, Hürtgen M. Video-assisted mediastinoscopic lymphadenectomy (VAMLA). In: Zieliński M, Rami-Porta R. editors. The Transcervical Approach in Thoracic Surgery. Heidelberg: Springer-Verlag, 2014:89-99.
LinkOut - more resources
Full Text Sources