

Apheresis therapies for NMOSD attacks: A retrospective study of 207 therapeutic interventions
- PMID: 30345331
- PMCID: PMC6192689
- DOI: 10.1212/NXI.0000000000000504
Apheresis therapies for NMOSD attacks: A retrospective study of 207 therapeutic interventions
Abstract
Objective: To analyze whether 1 of the 2 apheresis techniques, therapeutic plasma exchange (PE) or immunoadsorption (IA), is superior in treating neuromyelitis optica spectrum disorder (NMOSD) attacks and to identify predictive factors for complete remission (CR).
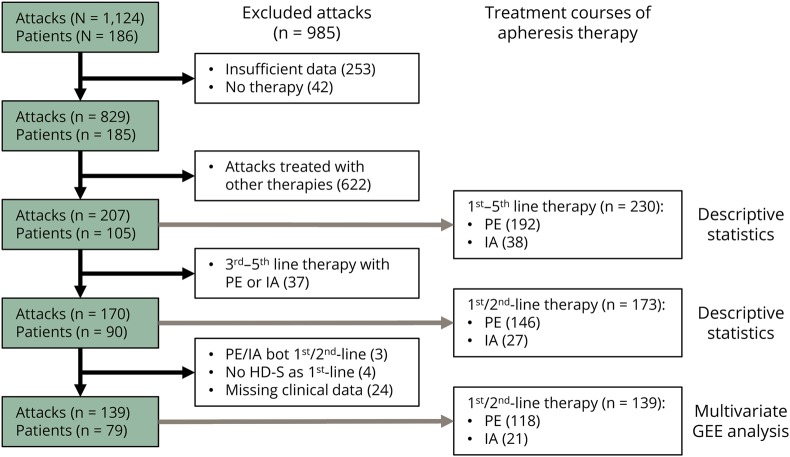
Methods: This retrospective cohort study was based on the registry of the German Neuromyelitis Optica Study Group, a nationwide network established in 2008. It recruited patients with neuromyelitis optica diagnosed according to the 2006 Wingerchuk criteria or with aquaporin-4 (AQP4-ab)-antibody-seropositive NMOSD treated at 6 regional hospitals and 16 tertiary referral centers until March 2013. Besides descriptive data analysis of patient and attack characteristics, generalized estimation equation (GEE) analyses were applied to compare the effectiveness of the 2 apheresis techniques. A GEE model was generated to assess predictors of outcome.
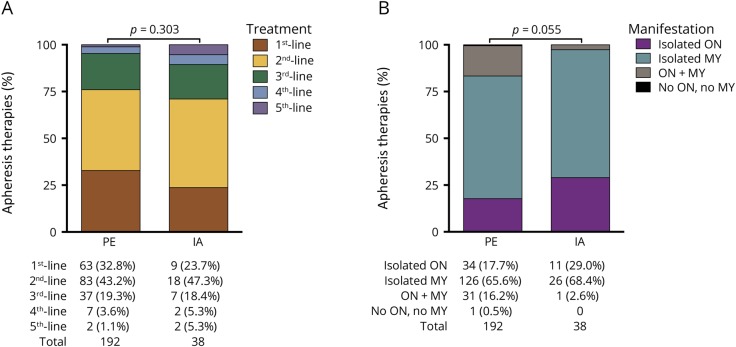
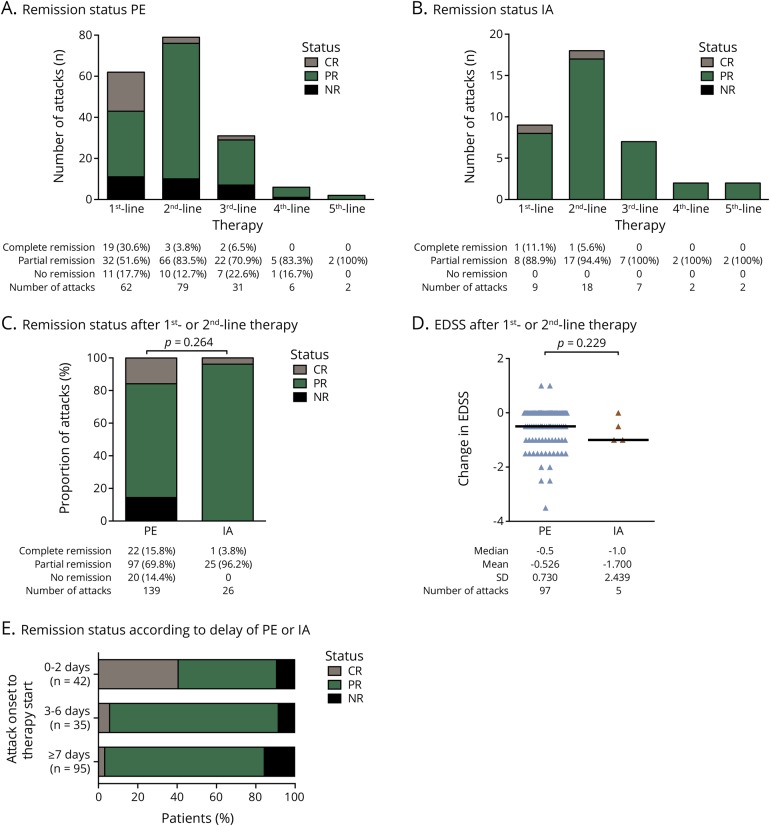
Results: Two hundred and seven attacks in 105 patients (87% AQP4-ab-antibody seropositive) were treated with at least 1 apheresis therapy. Neither PE nor IA was proven superior in the therapy of NMOSD attacks. CR was only achieved with early apheresis therapy. Strong predictors for CR were the use of apheresis therapy as first-line therapy (OR 12.27, 95% CI: 1.04-144.91, p = 0.047), time from onset of attack to start of therapy in days (OR 0.94, 95% CI: 0.89-0.99, p = 0.014), the presence of AQP4-ab-antibodies (OR 33.34, 95% CI: 1.76-631.17, p = 0.019), and monofocal attack manifestation (OR 4.71, 95% CI: 1.03-21.62, p = 0.046).
Conclusions: Our findings suggest early use of an apheresis therapy in NMOSD attacks, particularly in AQP4-ab-seropositive patients. No superiority was shown for one of the 2 apheresis techniques.
Classification of evidence: This study provides Class IV evidence that for patients with NMOSD, neither PE nor IA is superior in the treatment of attacks.
Figures
Comment in
- e510 doi: 10.1212/NXI.0000000000000510
References
-
- Kleiter I, Gahlen A, Borisow N, et al. Neuromyelitis optica: evaluation of 871 attacks and 1153 treatment courses. Ann Neurol 2016;79:206–216. - PubMed
-
- Bronzlik P, Toto S, Kielstein J, Schmidt B, Stangel M, Trebst C. Therapeutic plasma exchange and immunoadsorption therapy in neurological diseases. Eur Neu J 2011;3:56–61.
-
- Braun N, Bosch T. Immunoadsorption, current status and future developments. Expert Opin Investig Drugs 2000;9:2017–2038. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials