

Viral and other therapies for recurrent glioblastoma: is a 24-month durable response unusual?
- PMID: 30346600
- PMCID: PMC6303472
- DOI: 10.1093/neuonc/noy170
Viral and other therapies for recurrent glioblastoma: is a 24-month durable response unusual?
Abstract
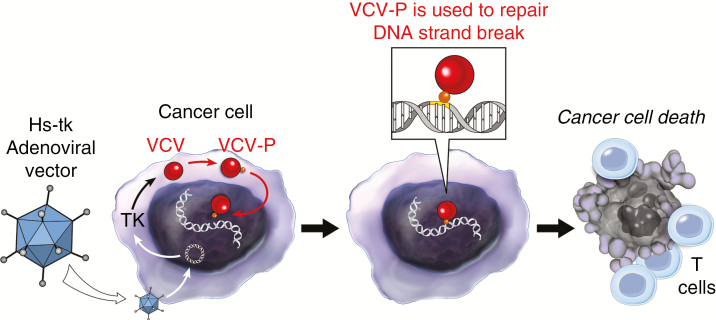
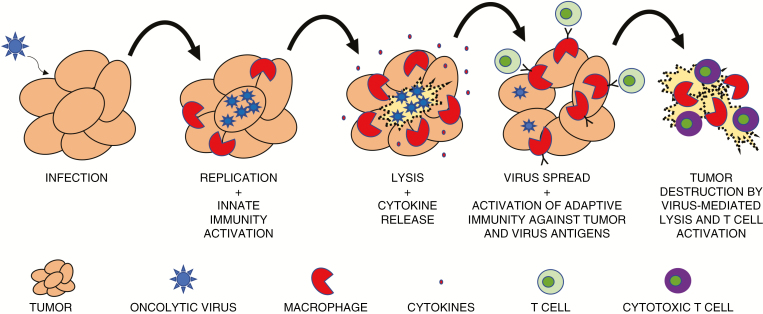
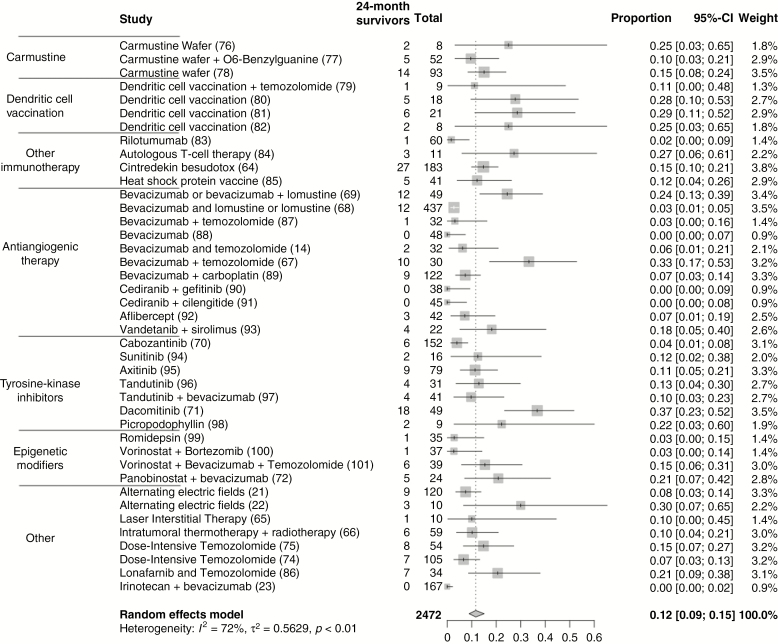
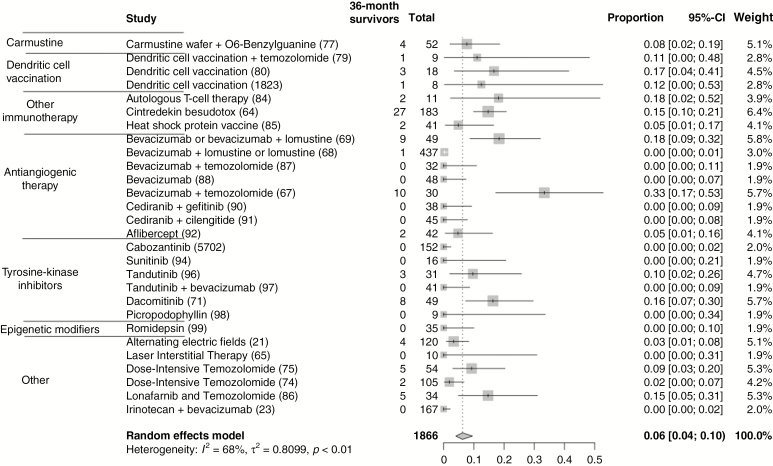
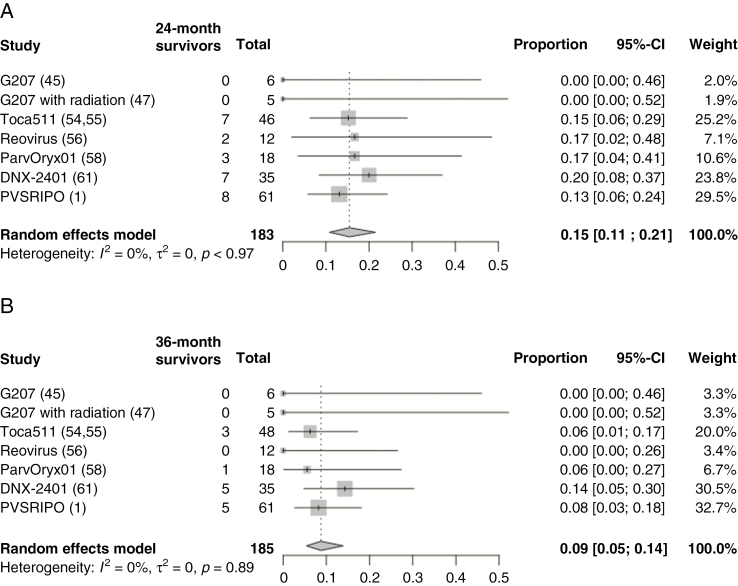
A phase I trial of an engineered poliovirus for the treatment of recurrent glioblastoma (GBM) has attracted attention due to 8 survivors reaching the 24-month and 5 reaching the 36-month survival landmarks.1 Genetically engineered viruses (oncolytic viruses) have been in trials for GBM for almost two decades.2 These replication-competent (tumor-selective, oncolytic, replication-conditional) viruses or replication-defective viral vectors (gene therapy) deliver cytotoxic payloads to tumors, leading to immunogenic death and intratumoral inflammatory responses. This transforms the tumor microenvironment from immunologically naïve ("cold") to inflamed ("hot"), increasing immune cell recognition of tumor antigens and the durable responses observed in virotherapy.3,4 Several current and past virotherapy trials have reported a "tail" of apparent responders at the 24-month landmark. Other modalities have also reported a "tail" of seemingly long-term survivors. These trials seem to show that these responder "tails" characterize a defined subset of GBM patients.
Figures
References
-
- Lawler SE, Speranza MC, Cho CF, Chiocca EA. Oncolytic Viruses in Cancer Treatment: A Review. JAMA Oncol. 2017;3(6):841–849. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. ; European Organisation for Research and Treatment of Cancer Brain Tumor and Radiotherapy Groups; National Cancer Institute of Canada Clinical Trials Group Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
