

Effect of Cricoid Pressure Compared With a Sham Procedure in the Rapid Sequence Induction of Anesthesia: The IRIS Randomized Clinical Trial
- PMID: 30347104
- PMCID: PMC6439856
- DOI: 10.1001/jamasurg.2018.3577
Effect of Cricoid Pressure Compared With a Sham Procedure in the Rapid Sequence Induction of Anesthesia: The IRIS Randomized Clinical Trial
Erratum in
-
Error in Byline.JAMA Surg. 2019 Jan 1;154(1):96. doi: 10.1001/jamasurg.2018.5449. JAMA Surg. 2019. PMID: 30649149 Free PMC article. No abstract available.
Abstract
Importance: The use of cricoid pressure (Sellick maneuver) during rapid sequence induction (RSI) of anesthesia remains controversial in the absence of a large randomized trial.
Objective: To test the hypothesis that the incidence of pulmonary aspiration is not increased when cricoid pressure is not performed.
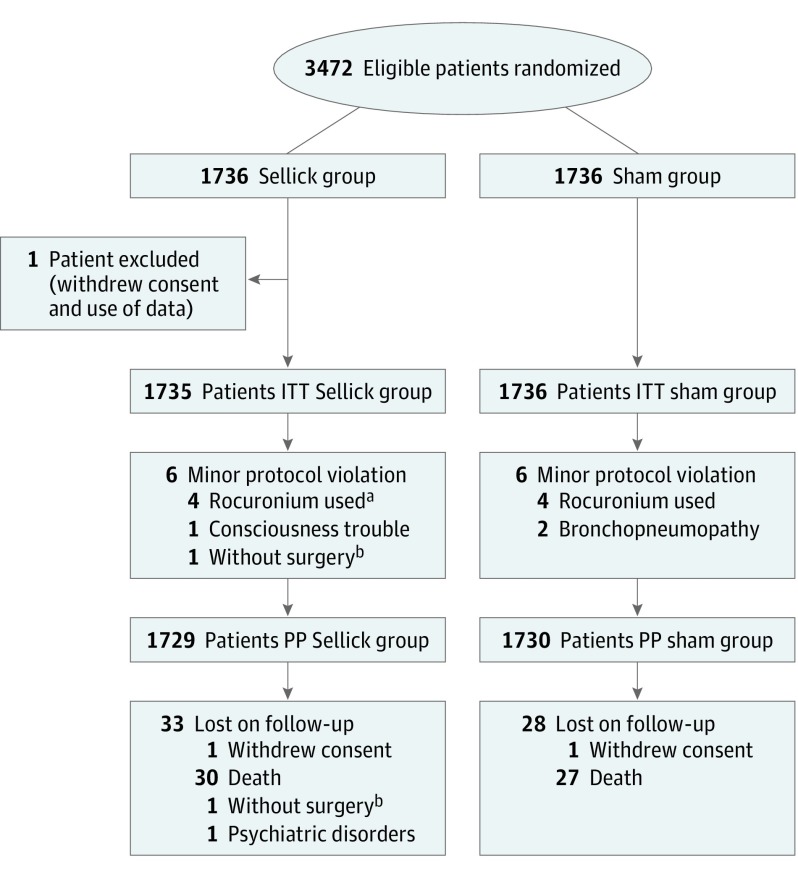
Design, setting, and participants: Randomized, double-blind, noninferiority trial conducted in 10 academic centers. Patients undergoing anesthesia with RSI were enrolled from February 2014 until February 2017 and followed up for 28 days or until hospital discharge (last follow-up, February 8, 2017).
Interventions: Patients were assigned to a cricoid pressure (Sellick group) or a sham procedure group.
Main outcomes and measures: Primary end point was the incidence of pulmonary aspiration (at the glottis level during laryngoscopy or by tracheal aspiration after intubation). It was hypothesized that the sham procedure would not be inferior to the cricoid pressure. The secondary end points were related to pulmonary aspiration, difficult tracheal intubation, and traumatic complications owing to the tracheal intubation or cricoid pressure.
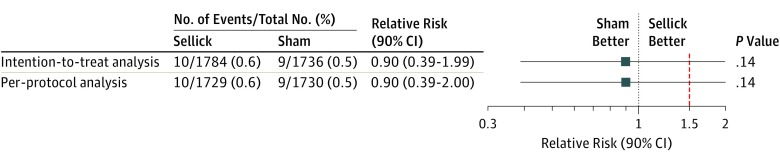
Results: Of 3472 patients randomized, mean (SD) age was 51 (19) years and 1777 (51%) were men. The primary end point, pulmonary aspiration, occurred in 10 patients (0.6%) in the Sellick group and in 9 patients (0.5%) in the sham group. The upper limit of the 1-sided 95% CI of relative risk was 2.00, exceeding 1.50, failing to demonstrate noninferiority (P = .14). The risk difference was -0.06% (2-sided 95% CI, -0.57 to 0.42) in the intent-to-treat population and -0.06% (2-sided 95% CI, -0.56 to 0.43) in the per protocol population. Secondary end points were not significantly different among the 2 groups (pneumonia, length of stay, and mortality), although the comparison of the Cormack and Lehane grade (Grades 3 and 4, 10% vs 5%; P <.001) and the longer intubation time (Intubation time >30 seconds, 47% vs 40%; P <.001) suggest an increased difficulty of tracheal intubation in the Sellick group.
Conclusions and relevance: This large randomized clinical trial performed in patients undergoing anesthesia with RSI failed to demonstrate the noninferiority of the sham procedure in preventing pulmonary aspiration. Further studies are required in pregnant women and outside the operating room.
Trial registration: ClinicalTrials.gov Identifier: NCT02080754.
Conflict of interest statement
Figures
Comment in
-
Is 30 Newtons of Prevention Worth a Pound of a Cure?-Cricoid Pressure.JAMA Surg. 2019 Jan 1;154(1):18. doi: 10.1001/jamasurg.2018.3590. JAMA Surg. 2019. PMID: 30347028 No abstract available.
-
Utility of Cricoid Pressure.JAMA Surg. 2019 Jun 1;154(6):561-562. doi: 10.1001/jamasurg.2018.5846. JAMA Surg. 2019. PMID: 30810724 No abstract available.
-
Utility of Cricoid Pressure.JAMA Surg. 2019 Jun 1;154(6):562. doi: 10.1001/jamasurg.2018.5847. JAMA Surg. 2019. PMID: 30810725 No abstract available.
-
Utility of Cricoid Pressure.JAMA Surg. 2019 Jun 1;154(6):562-563. doi: 10.1001/jamasurg.2018.5848. JAMA Surg. 2019. PMID: 30810726 No abstract available.
-
Utility of Cricoid Pressure.JAMA Surg. 2019 Jun 1;154(6):563-564. doi: 10.1001/jamasurg.2018.5850. JAMA Surg. 2019. PMID: 30810730 No abstract available.
-
Utility of Cricoid Pressure-Reply.JAMA Surg. 2019 Jun 1;154(6):564-565. doi: 10.1001/jamasurg.2018.5851. JAMA Surg. 2019. PMID: 30810731 No abstract available.
-
Utility of Cricoid Pressure.JAMA Surg. 2019 Jun 1;154(6):563. doi: 10.1001/jamasurg.2018.5849. JAMA Surg. 2019. PMID: 30810736 No abstract available.
References
-
- Warner MA, Warner ME, Weber JG. Clinical significance of pulmonary aspiration during the perioperative period. Anesthesiology. 1993;78(1):56-62. - PubMed
-
- Olsson GL, Hallen B, Hambraeus-Jonzon K. Aspiration during anaesthesia: a computer-aided study of 185,358 anaesthetics. Acta Anaesthesiol Scand. 1986;30(1):84-92. - PubMed
-
- Thomas TA, Cooper GM. Why Mothers Die 2000-2002: The Sixth Report of the Confidential Enquiries into Maternal Deaths in the United Kingdom. London: RCOG; 2001:137-138.
-
- Langeron O, Birenbaum A, Le Saché F, Raux M. Airway management in obese patient. Minerva Anestesiol. 2014;80(3):382-392. - PubMed
-
- Martin LD, Mhyre JM, Shanks AM, Tremper KK, Kheterpal S. 3,423 emergency tracheal intubations at a university hospital: airway outcomes and complications. Anesthesiology. 2011;114(1):42-48. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
