

Predicting 90-day and long-term mortality in octogenarians undergoing radical cystectomy
- PMID: 30348141
- PMCID: PMC6198515
- DOI: 10.1186/s12894-018-0402-z
Predicting 90-day and long-term mortality in octogenarians undergoing radical cystectomy
Abstract
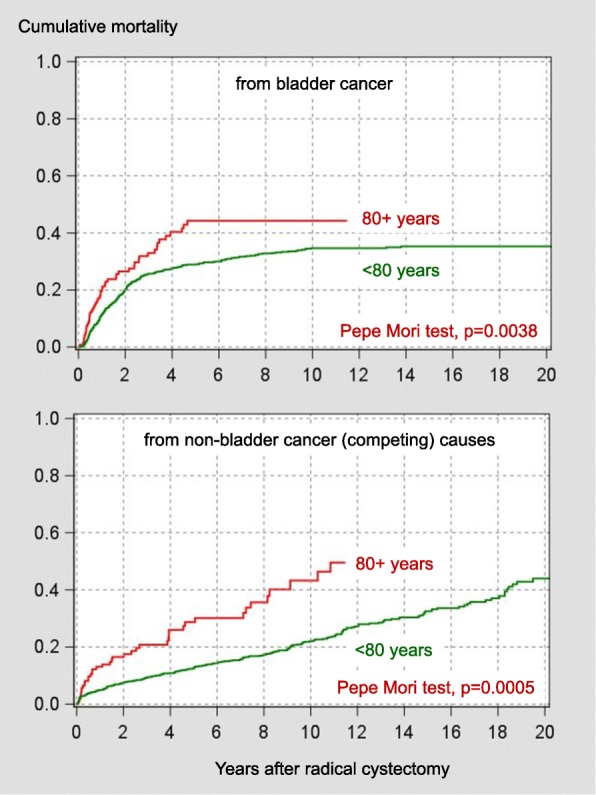
Background: Radical cystectomy bears a considerable perioperative mortality risk particularly in elderly patients. In this study, we searched for predictors of perioperative and long-term competing (non-bladder cancer) mortality in elderly patients selected for radical cystectomy.
Methods: We stratified 1184 consecutive patients who underwent radical cystectomy for high risk superficial or muscle-invasive urothelial or undifferentiated carcinoma of bladder into two groups (age < 80 years versus 80 years or older). Multivariable and cox proportional hazards models were used for data analysis.
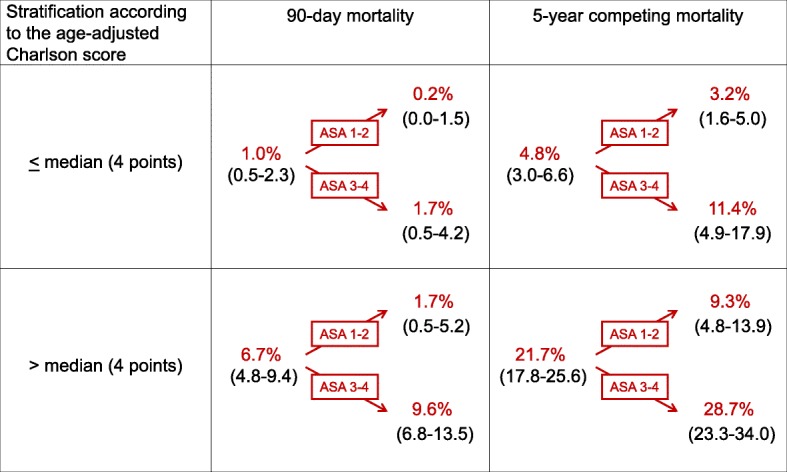
Results: Whereas Charlson score and the American Society of Anesthesiologists (ASA) physical status classification (but not age) were independent predictors of 90-day mortality in younger patients, only age predicted 90-day mortality in patients aged 80 years or older (odds ratio per year 1.24, p = 0.0422). Unlike in their younger counterparts, neither age nor Charlson score or ASA classification were predictors of long-term competing mortality in patients aged 80 years or older (hazard ratios 1.07-1.10, p values 0.21-0.77).
Conclusions: This data suggest that extrapolations of perioperative mortality or long-term mortality risks of younger patients to octogenarians selected for radical cystectomy should be used with caution. Concerning 90-day mortality, chronological age provided prognostic information whereas comorbidity did not.
Keywords: 90-day mortality; Age; Bladder cancer; Comorbidity; Competing mortality; Radical cystectomy.
Conflict of interest statement
Ethics approval and consent to participate
Institutional review board approval was obtained (Ethikkommission des Universitätsklinikums Dresden, EK84032009).
Consent for publication
Not applicable.
Competing interests
Competing financial interests: The authors declare that they have no competing interests..
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
