

Cardiac resynchronization therapy with a defibrillator (CRTd) in failing heart patients with type 2 diabetes mellitus and treated by glucagon-like peptide 1 receptor agonists (GLP-1 RA) therapy vs. conventional hypoglycemic drugs: arrhythmic burden, hospitalizations for heart failure, and CRTd responders rate
- PMID: 30348145
- PMCID: PMC6196445
- DOI: 10.1186/s12933-018-0778-9
Cardiac resynchronization therapy with a defibrillator (CRTd) in failing heart patients with type 2 diabetes mellitus and treated by glucagon-like peptide 1 receptor agonists (GLP-1 RA) therapy vs. conventional hypoglycemic drugs: arrhythmic burden, hospitalizations for heart failure, and CRTd responders rate
Abstract
Objectives: To evaluate clinical outcomes in patients with diabetes, treated by cardiac resynchronization therapy with a defibrillator (CRT-d), and glucagon-like peptide 1 receptor agonists (GLP-1 RA) in addition to conventional hypoglycemic therapy vs. CRTd patients under conventional hypoglycemic drugs.
Background: Patients with diabetes treated by CRTd experienced an amelioration of functional New York Association Heart class, reduction of hospital admissions, and mortality, in a percentage about 60%. However, about 40% of CRTd patients with diabetes experience a worse prognosis.
Materials and methods: We investigated the 12-months prognosis of CRTd patients with diabetes, previously treated with hypoglycemic drugs therapy (n 271) vs. a matched cohort of CRTd patients with diabetes treated with GLP-1 RA in addition to conventional hypoglycemic therapy (n 288).
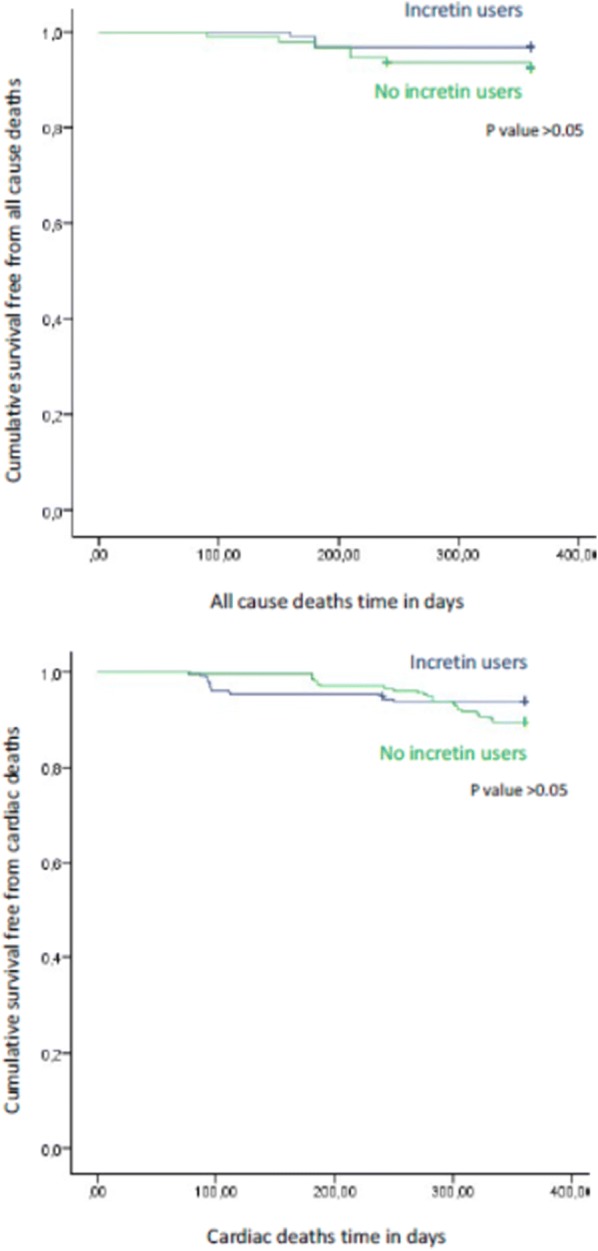
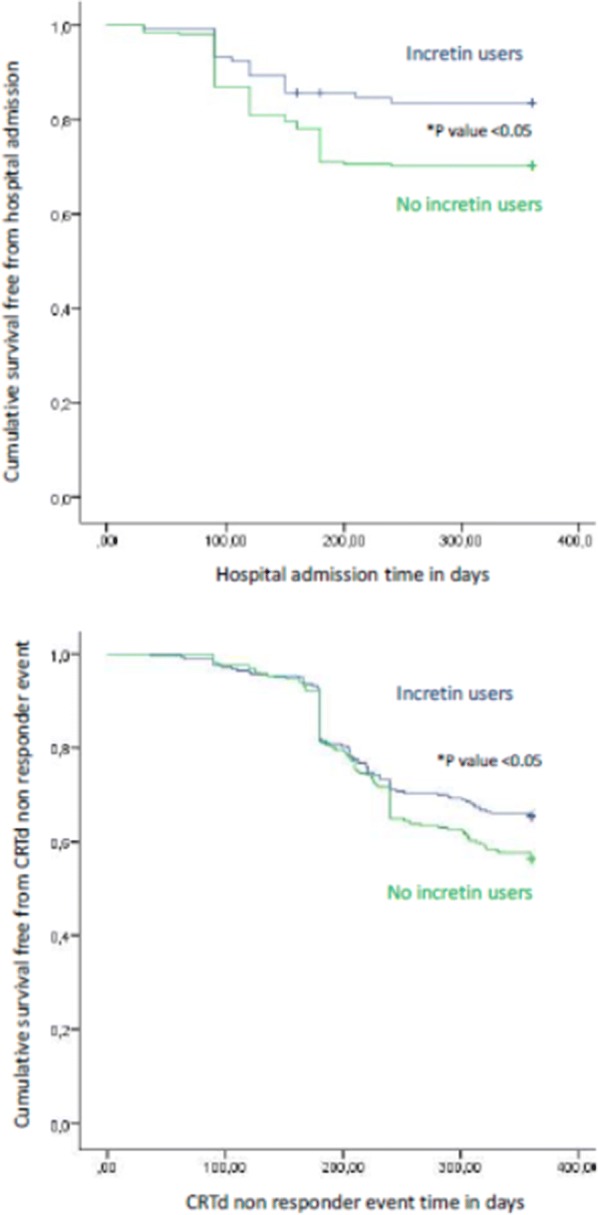
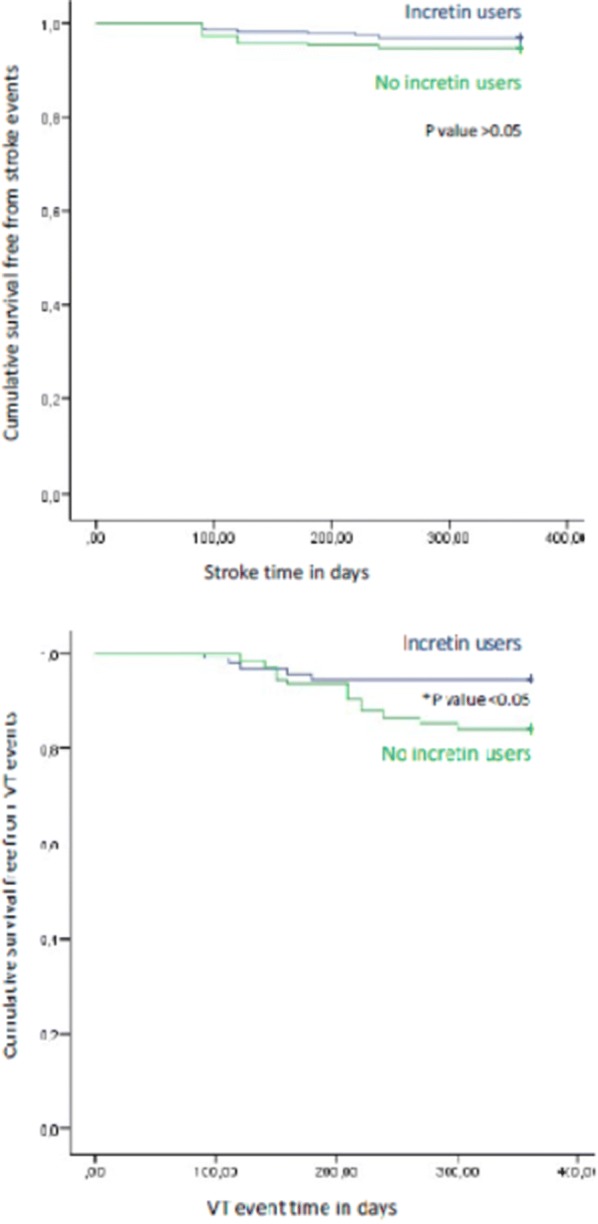
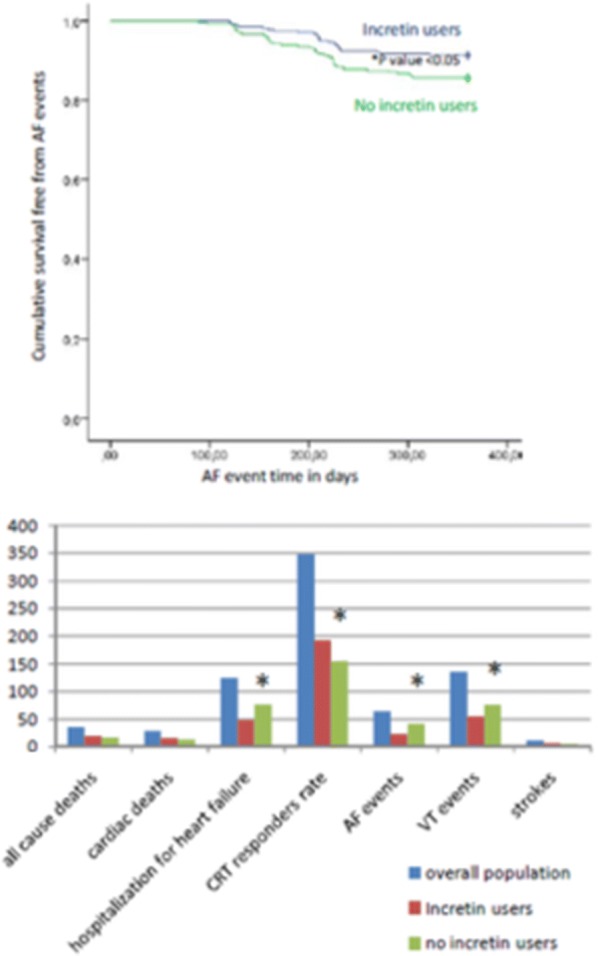
Results: At follow up CRTd patients with diabetes treated by GLP-1 RA therapy vs. CRTd patients with diabetes that did not receive GLP-1 RA therapy, experienced a significant reduction of NYHA class (p value < 0.05), associated to higher values of 6 min walking test (p value < 0.05), and higher rate of CRTd responders (p value < 0.05). GLP-1 RA patients vs. controls at follow up end experienced lower AF events (p value < 0.05), lower VT events (p value < 0.05), lower rate of hospitalization for heart failure worsening (p value < 0.05), and higher rate of CRTd responders (p value < 0.05). To date, GLP-1 RA therapy may predict a reduction of AF events (HR 0.603, CI [0.411-0.884]), VT events (HR 0.964, CI [0.963-0.992]), and hospitalization for heart failure worsening (HR 0.119, CI [0.028-0.508]), and a higher CRT responders rate (HR 3.707, CI [1.226-14.570]).
Conclusions: GLP-1 RA drugs in addition to conventional hypoglycemic therapy may significantly reduce systemic inflammation and circulating BNP levels in CRTd patients with diabetes, leading to a significant improvement of LVEF and of the 6 min walking test, and to a reduction of the arrhythmic burden. Consequently, GLP-1 RA drugs in addition to conventional hypoglycemic therapy may reduce hospital admissions for heart failure worsening, by increasing CRTd responders rate. Trial registration NCT03282136. Registered 9 December 2017 "retrospectively registered".
Figures
Similar articles
-
Multipolar pacing by cardiac resynchronization therapy with a defibrillators treatment in type 2 diabetes mellitus failing heart patients: impact on responders rate, and clinical outcomes.Cardiovasc Diabetol. 2017 Jun 9;16(1):75. doi: 10.1186/s12933-017-0554-2. Cardiovasc Diabetol. 2017. PMID: 28599667 Free PMC article. Clinical Trial.
-
Cardiac resynchronization therapy and its effects in patients with type 2 DIAbetes mellitus OPTimized in automatic vs. echo guided approach. Data from the DIA-OPTA investigators.Cardiovasc Diabetol. 2020 Nov 28;19(1):202. doi: 10.1186/s12933-020-01180-8. Cardiovasc Diabetol. 2020. PMID: 33248462 Free PMC article. Clinical Trial.
-
Amiodarone is associated with adverse outcomes in patients with sustained ventricular arrhythmias upgraded to cardiac resynchronization therapy-defibrillators.J Cardiovasc Electrophysiol. 2019 Mar;30(3):348-356. doi: 10.1111/jce.13828. Epub 2019 Jan 4. J Cardiovasc Electrophysiol. 2019. PMID: 30575185
-
Cardiac resynchronization is pro-arrhythmic in the absence of reverse ventricular remodelling: a systematic review and meta-analysis.Cardiovasc Res. 2018 Sep 1;114(11):1435-1444. doi: 10.1093/cvr/cvy182. Cardiovasc Res. 2018. PMID: 30010807
-
Major cardiovascular events, heart failure, and atrial fibrillation in patients treated with glucagon-like peptide-1 receptor agonists: An updated meta-analysis of randomized controlled trials.Nutr Metab Cardiovasc Dis. 2020 Jun 25;30(7):1106-1114. doi: 10.1016/j.numecd.2020.03.013. Epub 2020 Mar 25. Nutr Metab Cardiovasc Dis. 2020. PMID: 32448716
Cited by
-
Development of a Rapid Diagnostic Kit for Congestive Heart Failure Using Recombinant NT-proBNP Antigen.Medicina (Kaunas). 2021 Jul 25;57(8):751. doi: 10.3390/medicina57080751. Medicina (Kaunas). 2021. PMID: 34440957 Free PMC article.
-
High stress hyperglycemia ratio predicts adverse clinical outcome in patients with coronary three-vessel disease: a large-scale cohort study.Cardiovasc Diabetol. 2024 Jun 1;23(1):190. doi: 10.1186/s12933-024-02286-z. Cardiovasc Diabetol. 2024. PMID: 38824608 Free PMC article.
-
Feasibility and performance of catheter ablation with zero-fluoroscopy approach for regular supraventricular tachycardia in patients with structural and/or congenital heart disease.Medicine (Baltimore). 2019 Oct;98(41):e17333. doi: 10.1097/MD.0000000000017333. Medicine (Baltimore). 2019. PMID: 31593082 Free PMC article.
-
Oral Health Messiers: Diabetes Mellitus Relevance.Diabetes Metab Syndr Obes. 2021 Jul 1;14:3001-3015. doi: 10.2147/DMSO.S318972. eCollection 2021. Diabetes Metab Syndr Obes. 2021. PMID: 34234496 Free PMC article. Review.
-
Arrhythmic episodes in patients implanted with a cardioverter-defibrillator - results from the Prospective Study on Predictive Quality with Preferencing PainFree ATP therapies (4P).BMC Cardiovasc Disord. 2019 Jun 17;19(1):146. doi: 10.1186/s12872-019-1121-4. BMC Cardiovasc Disord. 2019. PMID: 31208342 Free PMC article.
References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Jr, Colvin MM, Drazner MH, Filippatos GS, Fonarow GC, Givertz MM, Hollenberg SM, Lindenfeld J, Masoudi FA, McBride PE, Peterson PN, Stevenson LW, Westlake C. 2017 ACC/AHA/HFSA focused update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70(6):776–803. doi: 10.1016/j.jacc.2017.04.025. - DOI - PubMed
-
- MacDonald MR, Petrie MC, Varyani F, Ostergren J, Michelson EL, Young JB, Solomon SD, Granger CB, Swedberg K, Yusuf S, Pfeffer MA, McMurray JJ, CHARM Investigators Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: assessment of reduction in mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29(11):1377–1385. doi: 10.1093/eurheartj/ehn153. - DOI - PubMed
-
- Sardu C, Barbieri M, Santamaria M, Giordano V, Sacra C, Paolisso P, Spirito A, Marfella R, Paolisso G, Rizzo MR. Multipolar pacing by cardiac resynchronization therapy with a defibrillators treatment in type 2 diabetes mellitus failing heart patients: impact on responders rate, and clinical outcomes. Cardiovasc Diabetol. 2017;16(1):75. doi: 10.1186/s12933-017-0554-2. - DOI - PMC - PubMed
-
- Filion KB, Azoulay L, Platt RW, Dahl M, Dormuth CR, Clemens KK, Hu N, Paterson JM, Targownik L, Turin TC, Udell JA, Ernst P, for the CNODES Investigators A multicenter observational study of GLP-1 agonist-based drugs and heart failure. N Engl J Med. 2016;374:1145–1154. doi: 10.1056/NEJMoa1506115. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
