

Application of the COM-B model to barriers and facilitators to chlamydia testing in general practice for young people and primary care practitioners: a systematic review
- PMID: 30348165
- PMCID: PMC6196559
- DOI: 10.1186/s13012-018-0821-y
Application of the COM-B model to barriers and facilitators to chlamydia testing in general practice for young people and primary care practitioners: a systematic review
Abstract
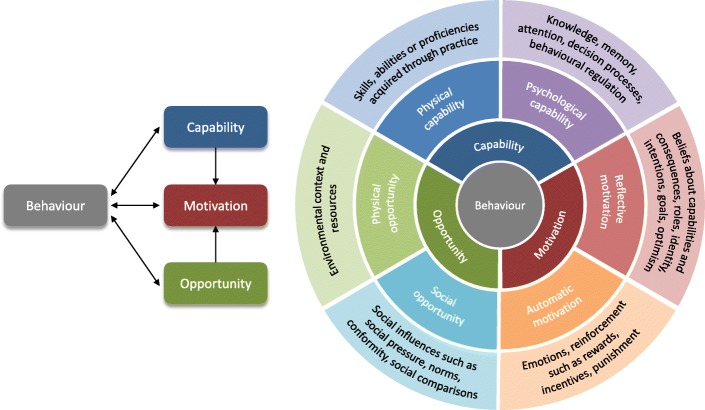
Background: Chlamydia is a major public health concern, with high economic and social costs. In 2016, there were over 200,000 chlamydia diagnoses made in England. The highest prevalence rates are found among young people. Although annual testing for sexually active young people is recommended, many do not receive testing. General practice is one ideal setting for testing, yet attempts to increase testing in this setting have been disappointing. The Capability, Opportunity, and Motivation Model of Behaviour (COM-B model) may help improve understanding of the underpinnings of chlamydia testing. The aim of this systematic review was to (1) identify barriers and facilitators to chlamydia testing for young people and primary care practitioners in general practice and (2) map facilitators and barriers onto the COM-B model.
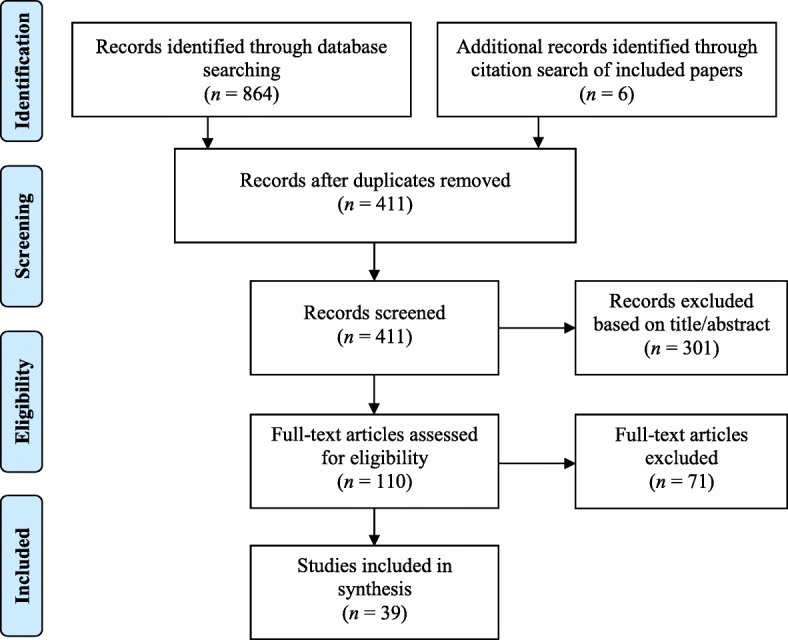
Methods: Qualitative, quantitative, and mixed methods studies published after 2000 were included. Seven databases were searched to identify peer-reviewed publications which examined barriers and facilitators to chlamydia testing in general practice. The quality of included studies was assessed using the Critical Appraisal Skills Programme. Data (i.e., participant quotations, theme descriptions, and survey results) regarding study design and key findings were extracted. The data was first analysed using thematic analysis, following this, the resultant factors were mapped onto the COM-B model components. All findings are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
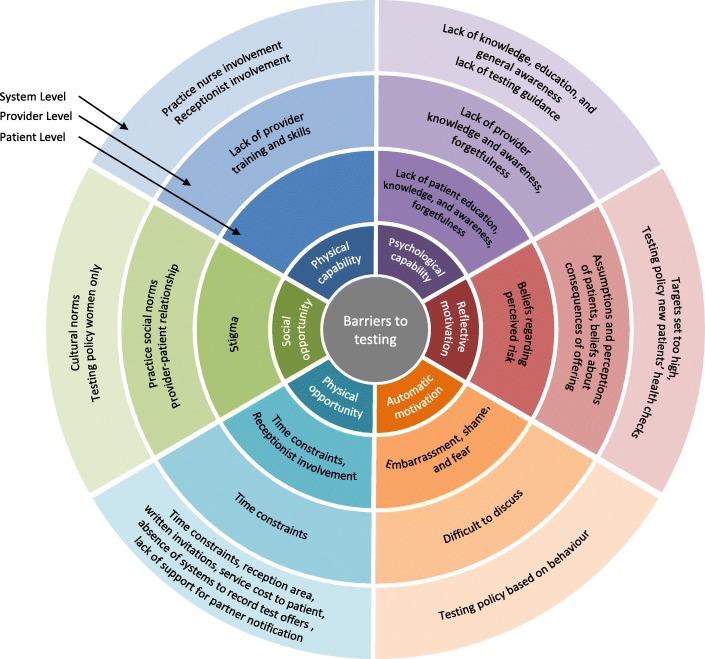
Results: Four hundred eleven papers were identified; 39 met the inclusion criteria. Barriers and facilitators were identified at the patient (e.g., knowledge), provider (e.g., time constraints), and service level (e.g., practice nurses). Factors were categorised into the subcomponents of the model: physical capability (e.g., practice nurse involvement), psychological capability (e.g.: lack of knowledge), reflective motivation (e.g., beliefs regarding perceived risk), automatic motivation (e.g., embarrassment and shame), physical opportunity (e.g., time constraints), social opportunity (e.g., stigma).
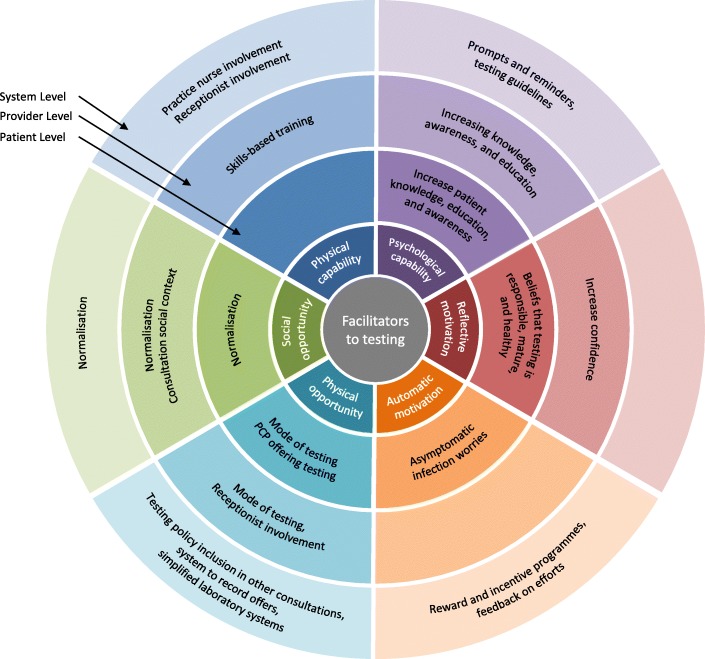
Conclusions: This systematic review provides a synthesis of the literature which acknowledges factors across multiple levels and components. The COM-B model provided the framework for understanding the complexity of chlamydia testing behaviour. While we cannot at this juncture state which component represents the most salient influence on chlamydia testing, across all three levels, multiple barriers and facilitators were identified relating psychological capability and physical and social opportunity. Implementation should focus on (1) normalisation, (2) communication, (3) infection-specific information, and (4) mode of testing. In order to increase chlamydia testing in general practice, a multifaceted theory- and evidence-based approach is needed.
Trial registration: PROSPERO CRD42016041786.
Keywords: Chlamydia; General practice; Implementation; Primary care; Systematic review; Young people.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
All authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Public Health England . Sexually transmitted infections and chlamydia screening in England, 2015. London: PHE; 2016.
-
- Hippisley-Cox J, Fenty J, Heaps M. Trends in consultation rates in general practice 1995 to 2006: analysis of the QRESEARCH database. London: QRESEARCH and The Information Centre for health and social care; 2007.
-
- Green Ruth, Kerry Sarah R, Reid Fiona, Hay Phillip E, Kerry Sally M, Aghaizu Adamma, Oakeshott Pippa. Where do sexually active female London students go to access healthcare? Evidence from the POPI (Prevention of Pelvic Infection) chlamydia screening trial. Sexually Transmitted Infections. 2012;88(5):382–385. doi: 10.1136/sextrans-2011-050452. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
