

The Assessment of Left Ventricle Function and Subclinical Atherosclerosis in Patients with Acute Myeloid Leukemia
- PMID: 30348722
- PMCID: PMC6365756
- DOI: 10.21873/invivo.11420
The Assessment of Left Ventricle Function and Subclinical Atherosclerosis in Patients with Acute Myeloid Leukemia
Abstract
Aim To assess the onset of early left ventricular (LV) systolic and diastolic function impairment and the subclinical atherosclerosis following chemotherapy in patients diagnosed with acute myeloid leukemia (AML).
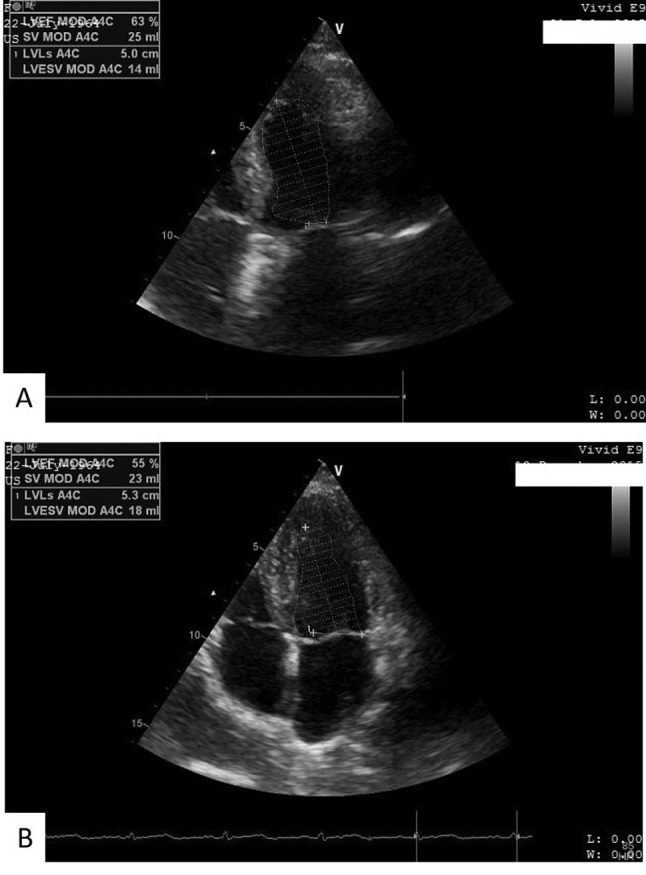
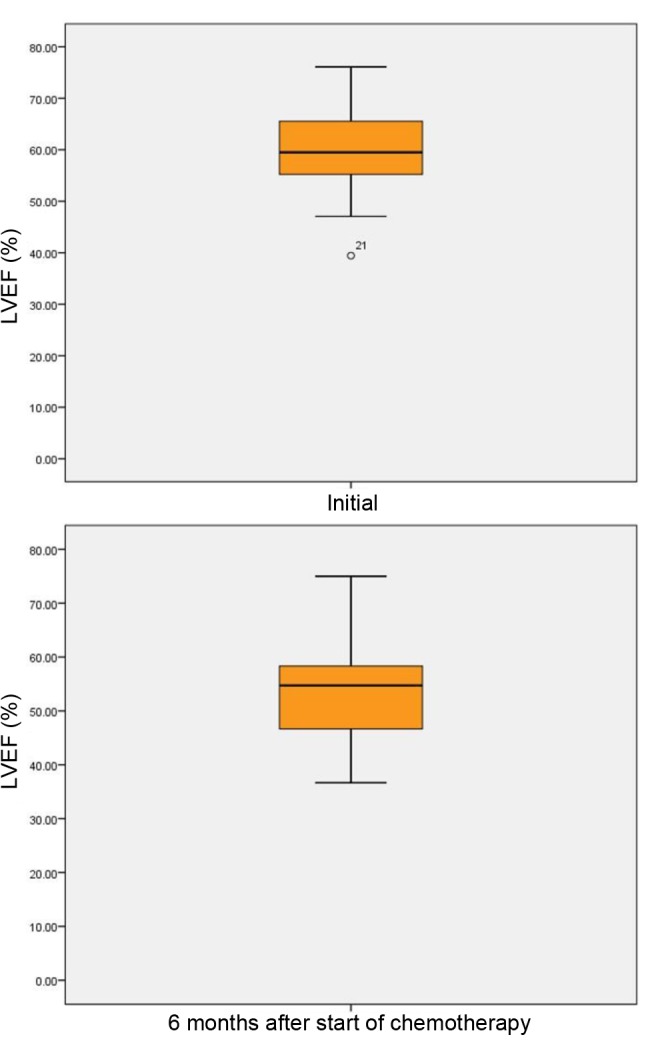
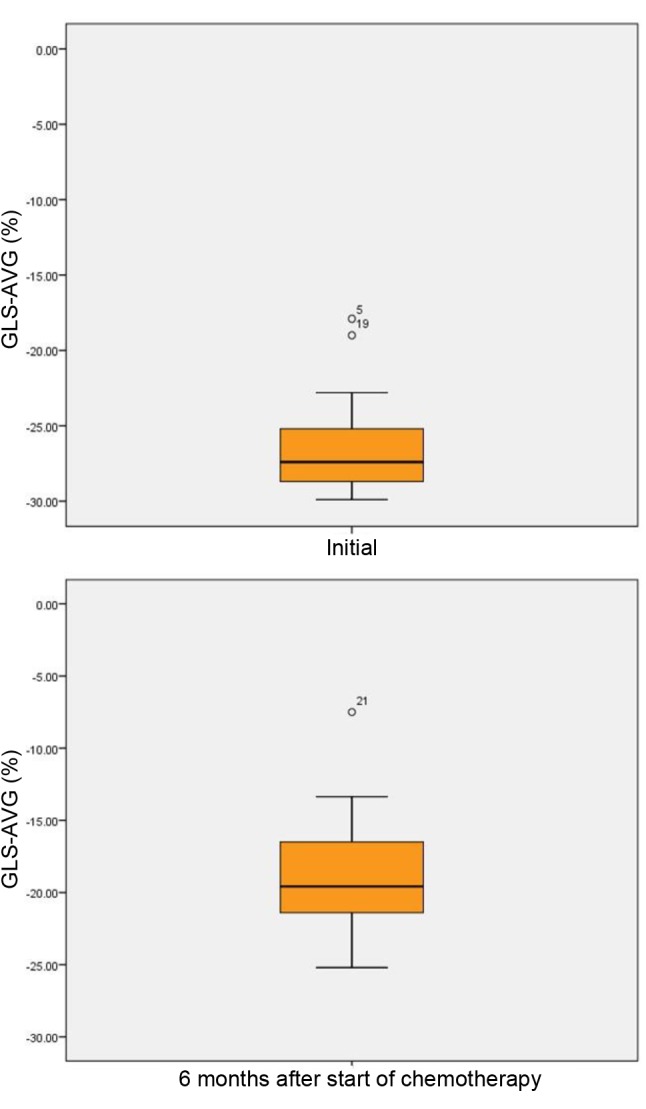
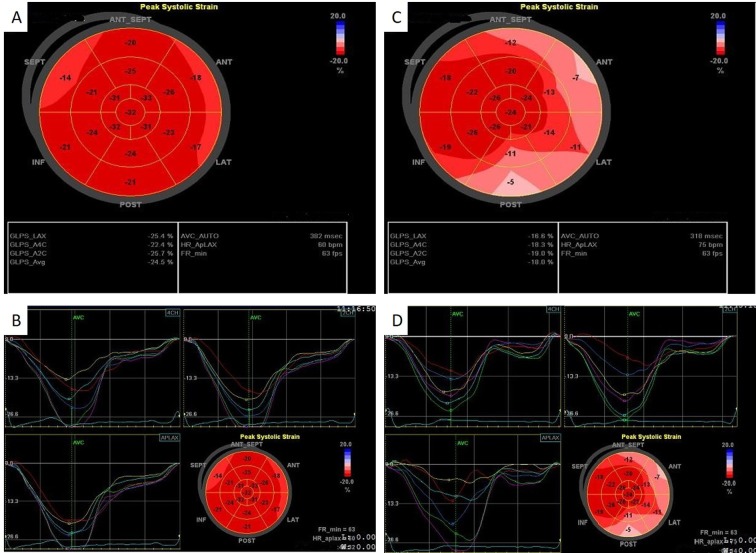
Materials and methods: Thirty patients diagnosed with AML with no cardiac history, having LV ejection fraction (LVEF) >50%, were evaluated at baseline and 6 months after starting four cycles of chemotherapy. We measured LV function, global longitudinal strain and subclinical atherosclerosis markers: intima-media thickness (IMT), arterial stiffness aortic pulse wave velocity (PWVAo) and ankle-brachial index (ABI).
Results: LVEF had decreased at 6 months after treatment initialization (p<0.001), the same changes being observed for LV fraction shortening (p<0.001), mitral annular plane systolic excursion and S' wave (p<0.001 and p<0.05). Bilateral IMT and PWVAo significantly increased, 12 out of 30 patients (40%) had LVEF ≤50% after 6 months of chemotherapy, five of them receiving daunorubicin at more than 500 mg/m2/injection.
Conclusion: LV function is impaired after 6 months of chemotherapy, with early changes of subclinical atherosclerosis becoming evident.
Keywords: Chemotherapy; LV function; arterial stiffness; cardiotoxicity; myocardial dysfunction; subclinical atherosclerosis.
Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved.
Figures
References
-
- Cardinale D, Colombo A, Lamantia G, Colombo N, Civelli M, De Giacomi G, Rubino M, Veglia F, Fiorentini C, Cipolla CM. Anthracycline-induced cardiomyopathy: clinical relevance and response to pharmacologic therapy. J Am Coll Cardiol. 2010;55(3):213–220. - PubMed
-
- Zamorano JL, Lancellotti P, Muñoz DR, Aboyans V, Asteggiano R, Galderisi M, Habib G, Lenihan DJ, Lip GY, Lyon AR, Fernandez TL, Mohty D, Piepoli MF, Tamargo J, Torbicki A, Suter TM. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines. Eur Heart J. 2016;37(36):2768–2801. - PubMed
-
- Simon A, Chironi G, Levenson J. Comparative performance of subclinical atherosclerosis tests in predicting coronary heart disease in asymptomatic individuals. Eur Heart J. 2007;28(24):2967–2971. - PubMed
-
- Döhner H, Estey EH, Amadori S, Appelbaum FR, Büchner T, Burnett AK, Dombret H, Fenaux P, Grimwade D, Larson RA, Lo-Coco F, Naoe T, Niederwieser D, Ossenkoppele GJ, Sanz MA, Sierra J, Tallman MS, Löwenberg B, Bloomfield CD. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European Leukemia Net. Blood. 2010;115(3):453–474. - PubMed
-
- Jain D, Russell RR, Schwartz RG, Panjrath GS, Aronow W. Cardiac complications of cancer therapy: Pathophysiology, identification, prevention, treatment, and future directions. Curr Cardiol Rep. 2017;19(5):36. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical