

Deep neural network improves fracture detection by clinicians
- PMID: 30348771
- PMCID: PMC6233134
- DOI: 10.1073/pnas.1806905115
Deep neural network improves fracture detection by clinicians
Abstract
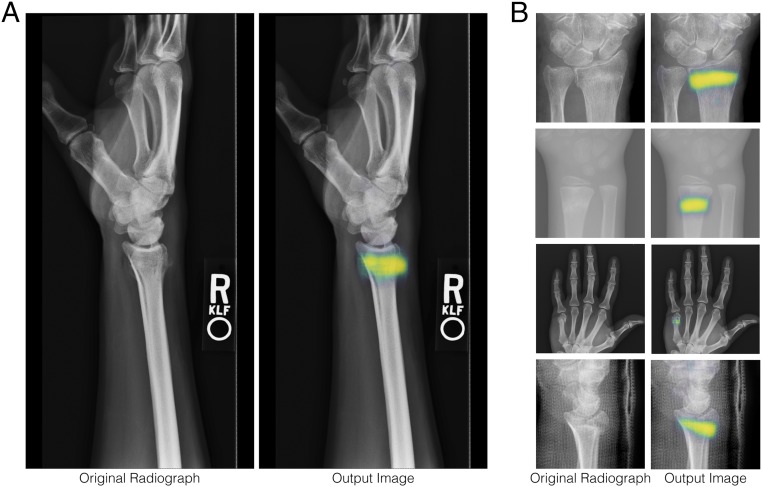
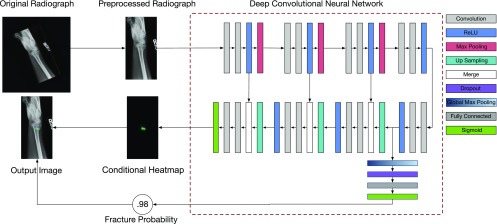
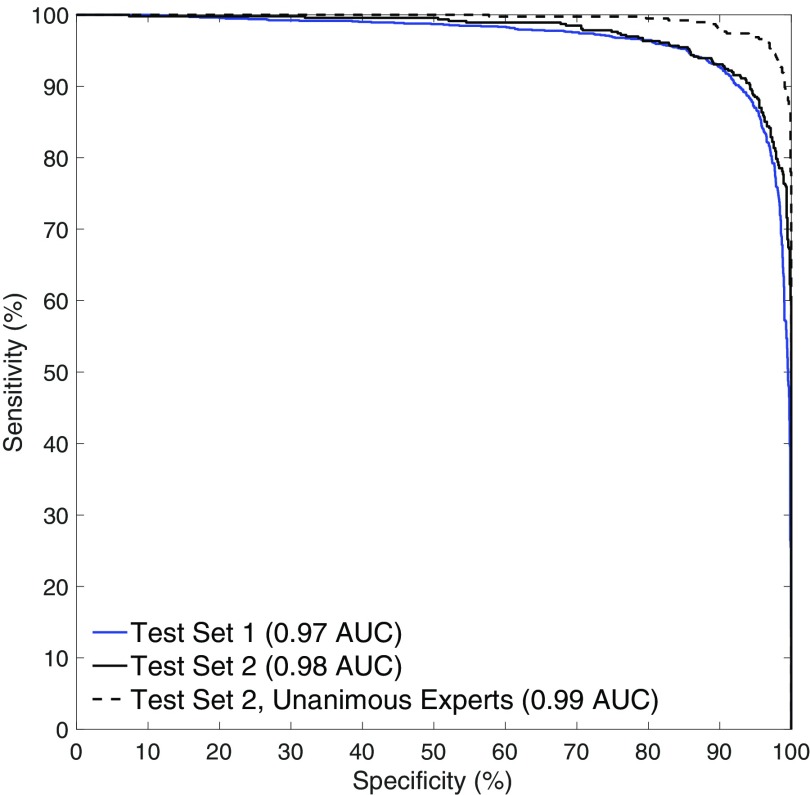
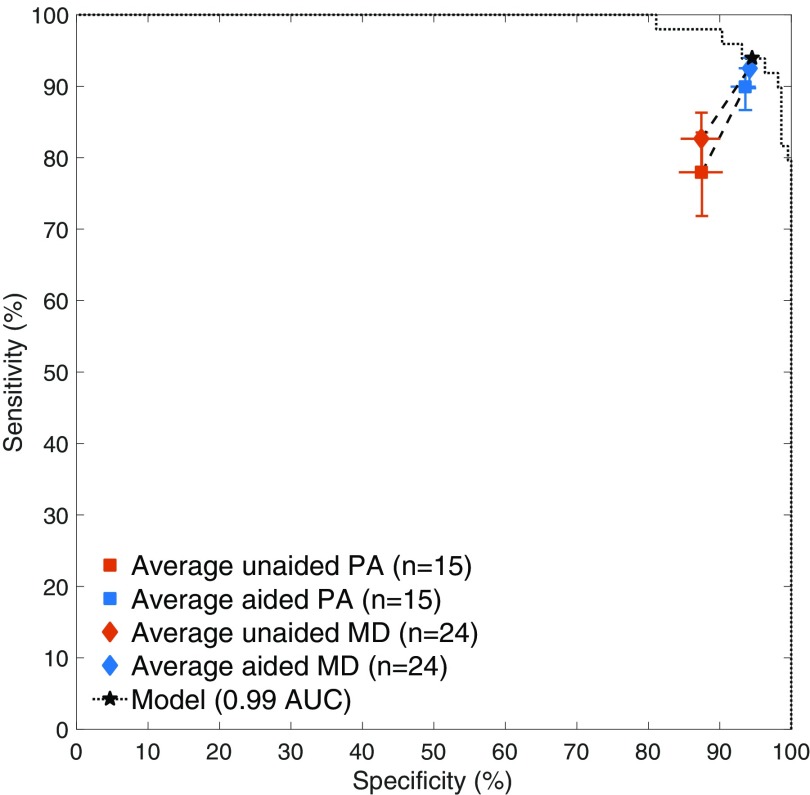
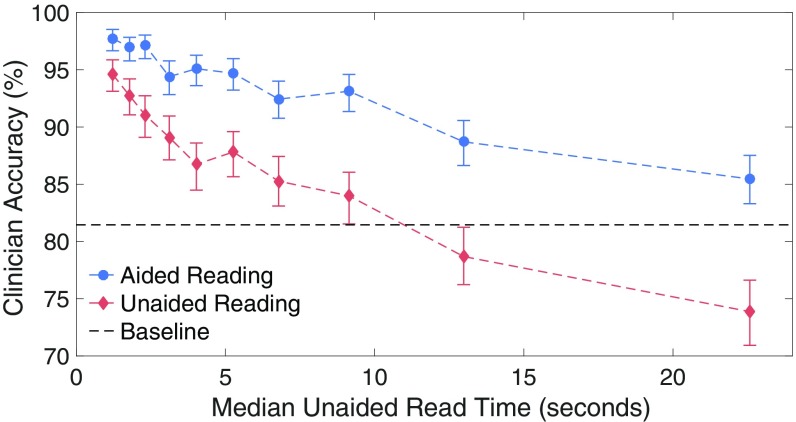
Suspected fractures are among the most common reasons for patients to visit emergency departments (EDs), and X-ray imaging is the primary diagnostic tool used by clinicians to assess patients for fractures. Missing a fracture in a radiograph often has severe consequences for patients, resulting in delayed treatment and poor recovery of function. Nevertheless, radiographs in emergency settings are often read out of necessity by emergency medicine clinicians who lack subspecialized expertise in orthopedics, and misdiagnosed fractures account for upward of four of every five reported diagnostic errors in certain EDs. In this work, we developed a deep neural network to detect and localize fractures in radiographs. We trained it to accurately emulate the expertise of 18 senior subspecialized orthopedic surgeons by having them annotate 135,409 radiographs. We then ran a controlled experiment with emergency medicine clinicians to evaluate their ability to detect fractures in wrist radiographs with and without the assistance of the deep learning model. The average clinician's sensitivity was 80.8% (95% CI, 76.7-84.1%) unaided and 91.5% (95% CI, 89.3-92.9%) aided, and specificity was 87.5% (95 CI, 85.3-89.5%) unaided and 93.9% (95% CI, 92.9-94.9%) aided. The average clinician experienced a relative reduction in misinterpretation rate of 47.0% (95% CI, 37.4-53.9%). The significant improvements in diagnostic accuracy that we observed in this study show that deep learning methods are a mechanism by which senior medical specialists can deliver their expertise to generalists on the front lines of medicine, thereby providing substantial improvements to patient care.
Keywords: CAD; X-ray; deep learning; fractures; radiology.
Copyright © 2018 the Author(s). Published by PNAS.
Conflict of interest statement
Conflict of interest statement: The authors are affiliated with Imagen Technologies, a startup company, the eventual products and services of which will be related to the subject matter of the article. The research was funded by Imagen Technologies. The authors own stock options in the company.
Figures
References
-
- Berlin L. Defending the “missed” radiographic diagnosis. Am J Roentgenol. 2001;176:317–322. - PubMed
-
- Kachalia A, et al. Missed and delayed diagnoses in the emergency department: A study of closed malpractice claims from 4 liability insurers. Ann Emerg Med. 2007;49:196–205. - PubMed
-
- Wei CJ, et al. Systematic analysis of missed extremity fractures in emergency radiology. Acta Radiologica. 2006;47:710–717. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
