

Case Reports
doi: 10.1002/ccr3.1785.
eCollection 2018 Oct.
Combined endodontic and periodontal management of a class 3 invasive cervical resorption in a mandibular first molar
Affiliations
- PMID: 30349717
- PMCID: PMC6186875
- DOI: 10.1002/ccr3.1785
Item in Clipboard
Case Reports
Combined endodontic and periodontal management of a class 3 invasive cervical resorption in a mandibular first molar
Clin Case Rep.
.
Abstract
Dental radiography and cone-beam computed tomography revealed the left mandibular first molar in a 68-year-old female patient with Heithersay Class 3 invasive cervical resorption (ICR). The inhibition of ICR progression and environmental improvement in and around the affected tooth through combined endodontic and periodontal treatments led to a favorable clinical outcome.
Keywords: cone‐beam computed tomography; free gingival graft; invasive cervical resorption; mineral trioxide aggregate; perforation repair.
Figures
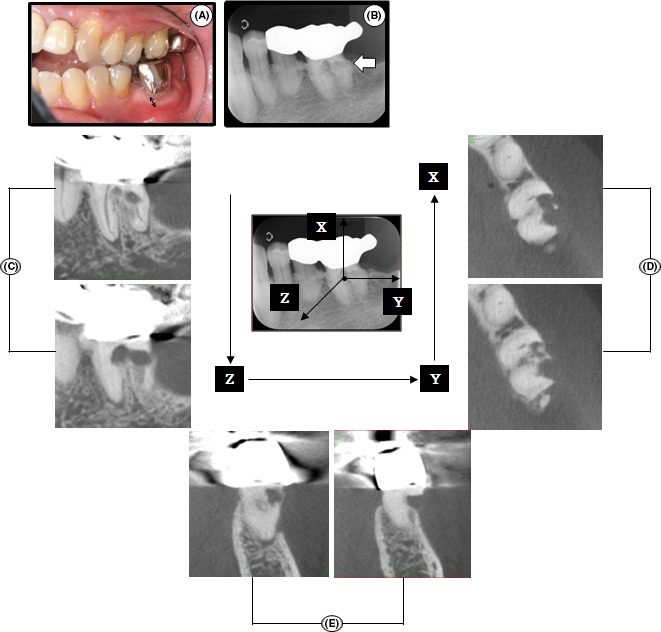
Intraoral photograph, dental radiograph, and CBCT images of tooth 36 at the first visit. A, Clinical view of left maxillary and mandibular quadrants. Attached gingiva was observed around tooth 36 (double‐headed arrow). B, Dental radiograph. An “irregular mottled” or “moth‐eaten” (irregular shape) appearance was observed (white arrow). C‐E, A series of CBCT images. Sagittal (C), axial (D), and coronal slices (E) clearly showed the resorptive lesion with an “outside‐in” appearance
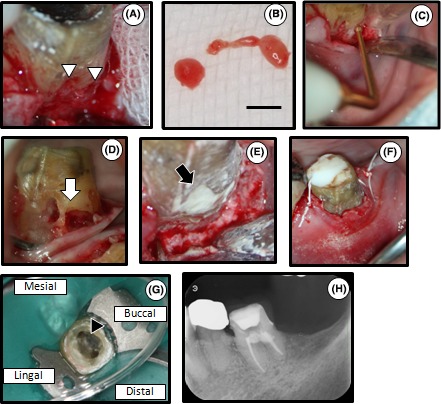
The first stage of treatment: removal of the granulomatous tissue, endodontic treatment and MTA filling of the defect. A, The surgical site. The cervical resorptive site was housed with the granulomatous tissue (white arrowheads). B, A part of the granulomatous tissue removed by the spoon excavator. Scale bar=3 mm. C, Complete removal of the granulomatous tissue by sonic instrument. D, Intraoral photograph after the removal of the granulomatous tissue. Pulp exposure measuring approximately 3 mm in diameter was observed at the resorptive site (white arrow). E, Filling of the resorptive site with MTA (black arrow). F, Tooth 36 after suturing. G, Location of root canal orifices and hardened MTA . Hardened MTA was observed (black arrowhead). The patient exhibited no clinical symptoms. H, Dental radiograph after root canal filling
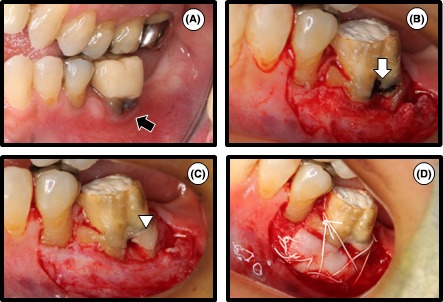
The second stage of treatment: free gingival graft. A, One month after root canal filling. Loss of attached gingiva was observed around tooth 36 with the temporary crown (black arrow). B, Clinical view of the partial‐thickness flap. Hardened MTA was observed (white arrow). C, Covering of the surface of hardened MTA with glass ionomer cement (white arrowhead). D, The graft was sutured at the recipient site to ensure immobilization. Graft tissue was harvested from the palate

Follow‐up. A, Intraoral photograph at the 3‐year follow‐up. A full metal crown was set on the tooth. Unusual views of the circumference of the gum were not accepted. An adequate width of attached gingiva was observed around tooth 36 (double‐headed arrow). B‐D, Dental radiographs were taken at three different horizontal angles at the 3‐year follow‐up (B, mesio‐eccentric projection; C, orthoradial projection; D, disto‐eccentric projection). Unusual views were not seen
References
-
- Heithersay GS. Treatment of invasive cervical resorption: an analysis of results using topical application of trichloroacetic acid, curettage, and restoration. Quintessence Int. 1999;30:96‐110. - PubMed
-
- Heithersay GS. Invasive cervical resorption. Endod Topics. 2004;7:73‐92.
-
- Heithersay GS. Management of tooth resorption. Aust Dent J. 2007;52:S105‐S121. - PubMed
-
- Hiremath H, Yakub SS, Metgud S, Bhagwat SV, Kulkarni S. Invasive cervical resorption: a case report. J Endod. 2007;33:999‐1003. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
