

Transcending Dimensions: a Comparative Analysis of Cloaca Imaging in Advancing the Surgeon's Understanding of Complex Anatomy
- PMID: 30350007
- PMCID: PMC6737109
- DOI: 10.1007/s10278-018-0139-y
Transcending Dimensions: a Comparative Analysis of Cloaca Imaging in Advancing the Surgeon's Understanding of Complex Anatomy
Abstract
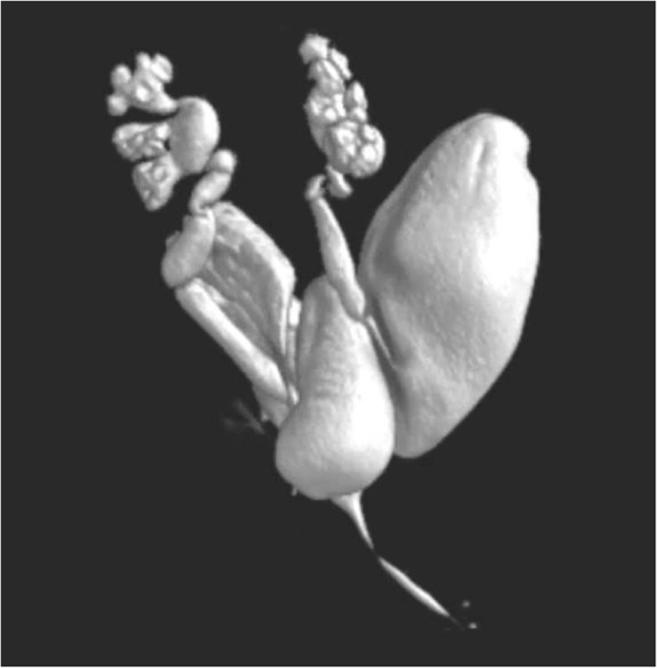
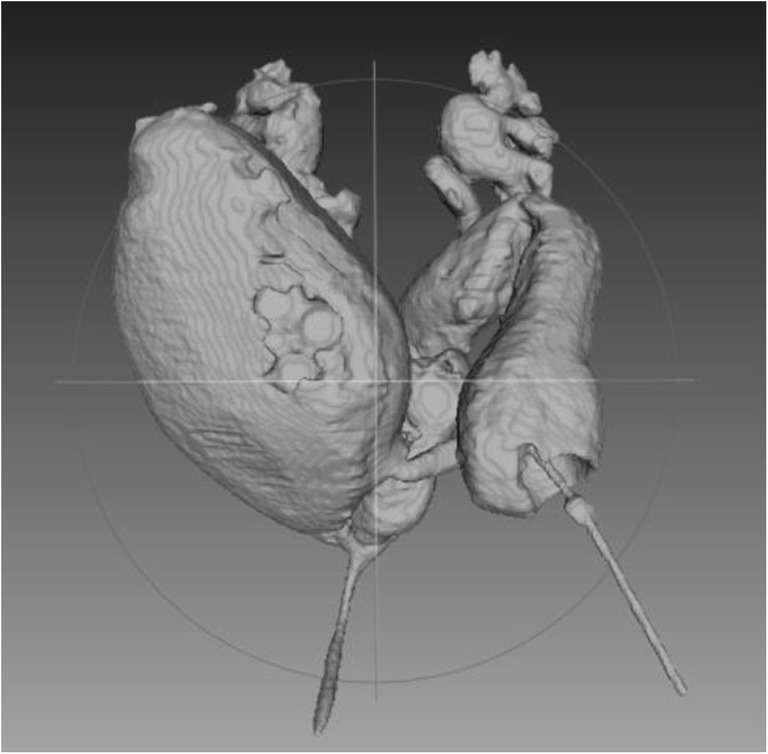
Surgeons have a steep learning capacity to understand 2-D images provided by conventional cloacagrams. Imaging advances now allow for 3-D reconstruction and 3-D models; but no evaluation of the value of these techniques exists in the literature. Therefore, we sought to determine if advances in 3-D imaging would benefit surgeons, lead to accelerated learning, and improve understanding for operative planning of a cloaca reconstruction. Questionnaires were used to assess the understanding of 2-D and 3-D images by pediatric surgical faculty and trainees. For the same case of a cloacal malformation, a 2D contrast study cloacagram, a 3D model rotatable CT scan reconstruction, a software enhanced 3D video animation (which allowed the observer to manipulate the structure in any orientation), and a printed physical 3D cloaca model that could be held in the observer's hand were employed. Logistic mixed effect models assessed whether the proportion of questions about the case that were answered correctly differed by imaging modality, and whether the proportion answered correctly differed between trainee and attending surgeons for any particular modality. Twenty-nine pediatric surgery trainees (27 pediatric general surgery and 2 pediatric urology surgery trainees) and 30 pediatric surgery and urology faculty participated. For trainees, the percentage of questions answered correctly was: 2-D 10.5%, 3-D PACS 46.7%, 3-D Enhanced 67.1%, and 3-D Printed 73.8%. For faculty, the total percentage of questions answered correctly was: 2-D 22.2%, 3-D PACS 54.8%, 3D Enhanced 66.2%, and 3-D printed 74.0%. The differences in rates of correctness across all four modalities were significant in both fellows and attendings (p < 0.001), with performance being lowest for the 2-D modality, and with increasing percentage of correct answers with each subsequent modality. The difference between trainees and attendings in correctness rate was significant only for the 2-D modality, with attendings answering correctly more often. The 2-D cloacagram, as the least complex model, was the most difficult to interpret. The more complex the modality, the more correct were the responses obtained from both groups. Trainees and attendings had similar levels of correct answers and understanding of the cloacagram for the more advanced modalities. Mental visualization skills of anatomy and complex 3-D spatial arrangements traditionally have taken years of experience to master. Now with novel surgical education resources of a 3-D cloacagram, a more quickly advancing skill is possible.
Keywords: 3D printing; Anorectal malformation; Cloaca; Surgical education.
Figures


Similar articles
-
Use of 3D reconstruction cloacagrams and 3D printing in cloacal malformations.J Pediatr Urol. 2017 Aug;13(4):395.e1-395.e6. doi: 10.1016/j.jpurol.2017.05.019. Epub 2017 Jun 20. J Pediatr Urol. 2017. PMID: 28673795
-
Introducing Cloacagram in Israel: Advancing Anatomical Assessment and Surgical Planning for Cloacal Malformations.Isr Med Assoc J. 2024 Oct;26(9):551-554. Isr Med Assoc J. 2024. PMID: 39397499
-
Measure twice and cut once: Comparing endoscopy and 3D cloacagram for the common channel and urethral measurements in patients with cloacal malformations.J Pediatr Surg. 2020 Feb;55(2):257-260. doi: 10.1016/j.jpedsurg.2019.10.045. Epub 2019 Nov 5. J Pediatr Surg. 2020. PMID: 31784103 Review.
-
Facilitating surgeon understanding of complex anatomy using a three-dimensional printed model.J Surg Res. 2017 Aug;216:18-25. doi: 10.1016/j.jss.2017.04.003. Epub 2017 Apr 21. J Surg Res. 2017. PMID: 28807205
-
Use of rotational fluoroscopy and 3-D reconstruction for pre-operative imaging of complex cloacal malformations.Semin Pediatr Surg. 2016 Apr;25(2):96-101. doi: 10.1053/j.sempedsurg.2015.11.008. Epub 2015 Nov 10. Semin Pediatr Surg. 2016. PMID: 26969233 Review.
Cited by
-
Application of 3D printing technology for pre-operative evaluation, education and informed consent in pediatric retroperitoneal tumors.Sci Rep. 2023 Jan 30;13(1):1671. doi: 10.1038/s41598-023-28423-4. Sci Rep. 2023. PMID: 36717595 Free PMC article.
-
Innovation in Urology: Three Dimensional Printing and Its Clinical Application.Front Surg. 2020 Jun 2;7:29. doi: 10.3389/fsurg.2020.00029. eCollection 2020. Front Surg. 2020. PMID: 32582760 Free PMC article. Review.
-
Cloacal Malformations: Technical Aspects of the Reconstruction and Factors Which Predict Surgical Complexity.Front Pediatr. 2019 Jun 14;7:240. doi: 10.3389/fped.2019.00240. eCollection 2019. Front Pediatr. 2019. PMID: 31259166 Free PMC article. Review.
-
Case report: Magnetic resonance imaging-based three-dimensional printing for reconstruction of complex cloacal malformations.Front Pediatr. 2023 Mar 7;11:1103401. doi: 10.3389/fped.2023.1103401. eCollection 2023. Front Pediatr. 2023. PMID: 36959843 Free PMC article.
-
Role of 3D printing technology in paediatric teaching and training: a systematic review.BMJ Paediatr Open. 2021 Dec;5(1):e001050. doi: 10.1136/bmjpo-2021-001050. BMJ Paediatr Open. 2021. PMID: 35290958 Free PMC article.
References
-
- Hermsen JL, Burke TM, Seslar SP et al. Scan, plan, print, practice, perform: Development and use of a patient specific 3-dimensional printed model in adult cardiac surgery. J Thorac Cardiovasc Surg. 2016 Aug 20. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
