

Three weeks of respiratory muscle endurance training improve the O2 cost of walking and exercise tolerance in obese adolescents
- PMID: 30350405
- PMCID: PMC6198139
- DOI: 10.14814/phy2.13888
Three weeks of respiratory muscle endurance training improve the O2 cost of walking and exercise tolerance in obese adolescents
Abstract
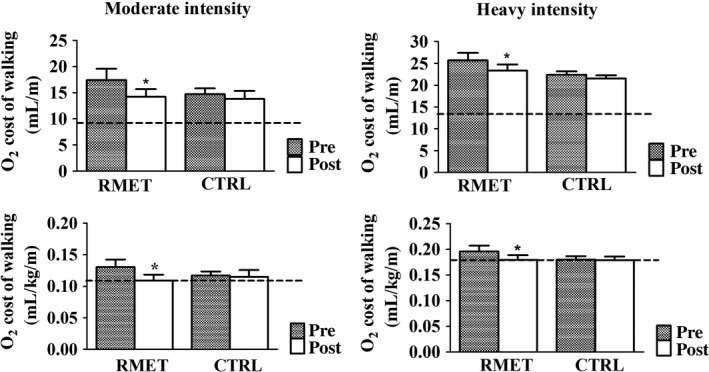
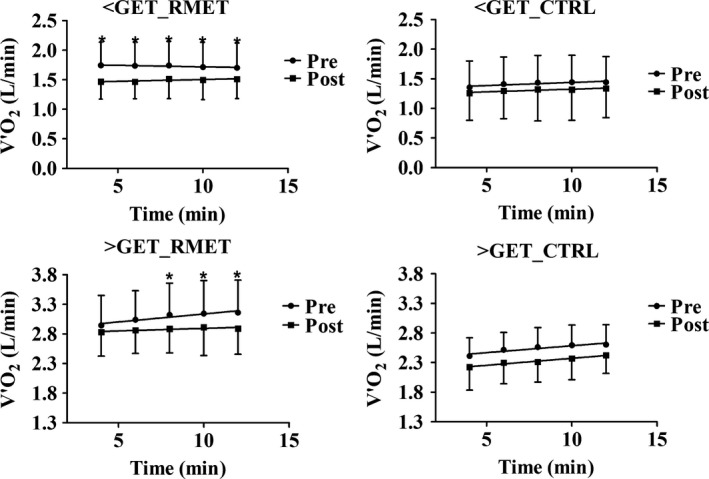
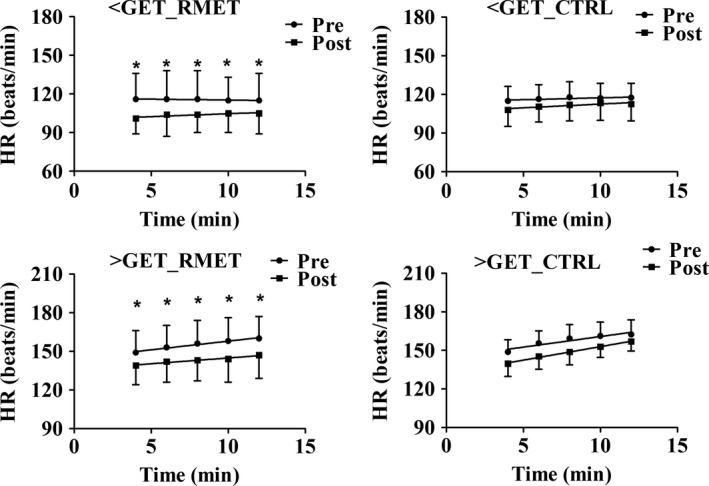
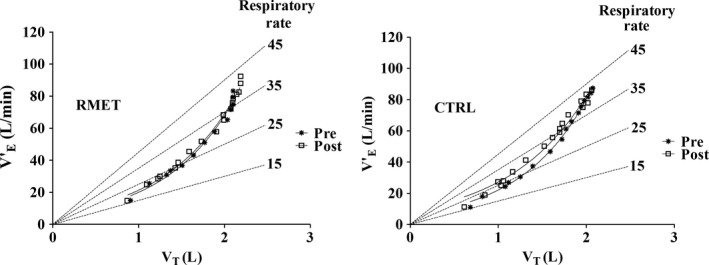
Obese adolescents (OB) have an increased O2 cost of exercise, attributable in part to an increased O2 cost of breathing. In a previous work a short (3-week) program of respiratory muscle endurance training (RMET) slightly reduced in OB the O2 cost of high-intensity cycling and improved exercise tolerance. We hypothesized that during treadmill walking the effects of RMET would be more pronounced than those observed during cycling. Sixteen OB (age 16.0 ± 0.8 years; body mass [BM] 127.7 ± 14.2 kg; body mass index 40.7 ± 4.0 kg/m2 ) underwent to 3-week RMET (n = 8) superimposed to a multidisciplinary BM reduction program, or (CTRL, n = 8) only to the latter. Heart rate (HR) and pulmonary O2 uptake ( O2 ) were measured during incremental exercise and 12-min constant work rate (CWR) walking at 60% (moderate-intensity, MOD) and 120% (heavy-intensity, HEAVY) of the gas exchange threshold (GET). The O2 cost of walking (aerobic energy expenditure per unit of covered distance) was calculated as O2 /velocity. BM decreased (~4-5 kg) both in CTRL and in RMET. O2 peak and GET were not affected by both interventions; the time to exhaustion increased following RMET. During MOD and HEAVY RMET decreased O2, the O2 cost of walking (MOD: 0.130 ± 0.033 mL/kg/m [before] vs. 0.109 ± 0.027 [after], P = 0.03; HEAVY: 0.196 ± 0.031 [before] vs. 0.180 ± 0.025 [after], P = 0.02), HR and rates of perceived exertion; no significant changes were observed in CTRL. In OB a short RMET program lowered the O2 cost of MOD and HEAVY walking and improved exercise tolerance. RMET could represent a useful adjunct in the control of obesity.
Keywords: O2 cost of breathing; O2 cost of walking; Obesity; respiratory muscle endurance training.
© 2018 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of The Physiological Society and the American Physiological Society.
Figures
Comment in
-
Breathing during exercise: There is no such thing as a free lunch.Exp Physiol. 2019 Sep;104(9):1333-1334. doi: 10.1113/EP087922. Epub 2019 Jul 30. Exp Physiol. 2019. PMID: 31325338 No abstract available.
References
-
- Beaver, W. L. , Wasserman K., and Whipp B. J.. 1986. A new method for detecting anaerobic threshold by gas exchange. J. Appl. Physiol. 60:2020–2027. - PubMed
-
- Cacciari, E. , Milani S., Balsamo A., Spada E., Bona G., Cavallo L., et al. 2006. Italian cross sectional growth charts for height weight and BMI (2 to 20 yr). J. Endocrinol. Invest. 29:581–593. - PubMed
-
- Coast, J. R. , Rasmussen S. A., Krause K. M., O'Kroy J. A., Loy R. A., and Rhodes J.. 1993. Ventilatory work and oxygen consumption during exercise and hyperventilation. J. Appl. Physiol. 74:793–798. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
