

FDG and FMISO PET-guided dose escalation with intensity-modulated radiotherapy in lung cancer
- PMID: 30352608
- PMCID: PMC6199734
- DOI: 10.1186/s13014-018-1147-2
FDG and FMISO PET-guided dose escalation with intensity-modulated radiotherapy in lung cancer
Abstract
Background: Concomitant chemo-radiotherapy is the reference treatment for non-resectable locally-advanced Non-Small Cell Lung Cancer (NSCLC). Increasing radiotherapy total dose in the whole tumour volume has been shown to be deleterious. Functional imaging with positron emission tomography (PET/CT) offers the potential to identify smaller and biologically meaningful target volumes that could be irradiated with larger doses without compromising Organs At Risk (OAR) tolerance. This study investigated four scenarios, based on 18FDG and 18F-miso PET/CT, to delineate the target volumes and derive radiotherapy plans delivering up to 74Gy.
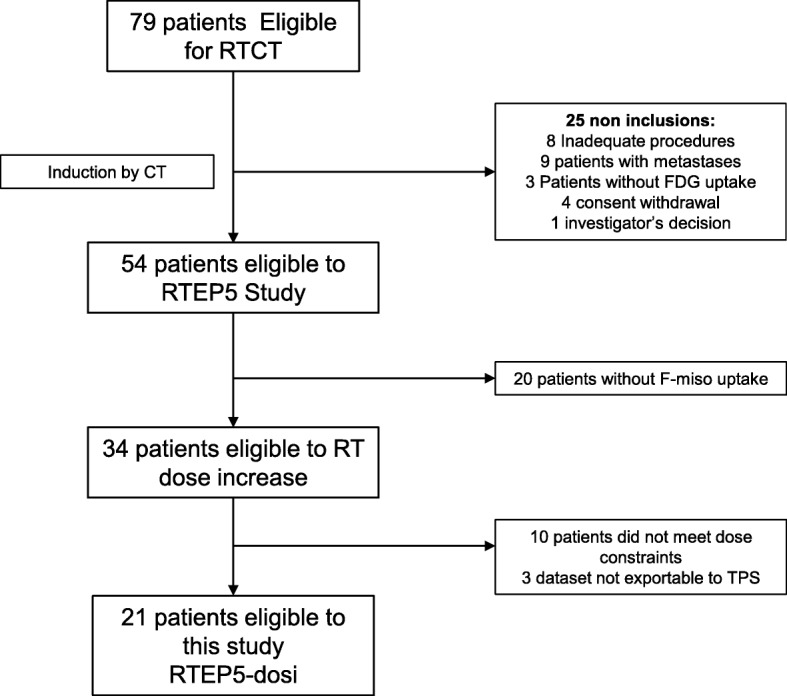
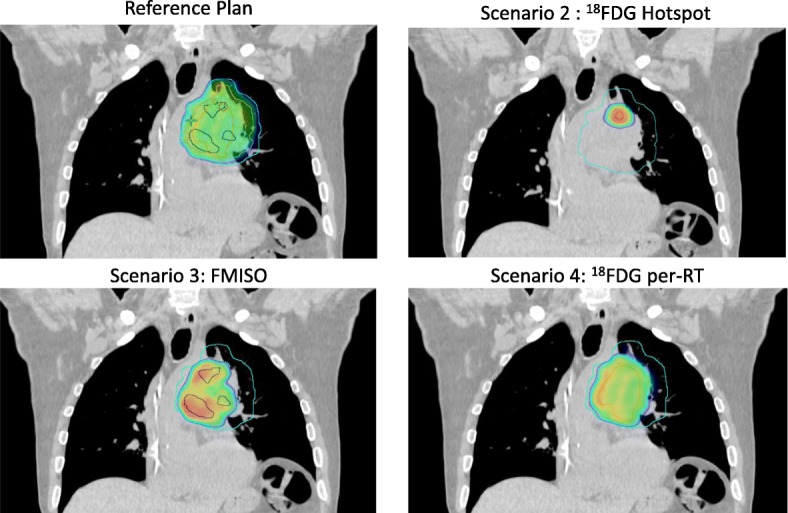
Method: Twenty-one NSCLC patients, selected from a prospective phase II trial, had 18FDG- and 18F-miso PET/CT before the start of radiotherapy and 18FDG PET/CT during the radiotherapy (42Gy). The plans were based planned on a standard plan delivering 66 Gy (plan 1) and on three different boost strategies to deliver 74Gy total dose in pre-treatment 18FDG hotspot (70% of SUVmax) (plan 2), pre-treatment 18F-miso target (SUVmax > 1.4) (plan 3) and per-treatment 18FDG residual (40% of SUVmax). (plan 4).
Results: The mean target volumes were 4.8 cc (± 1.1) for 18FDG hotspot, 38.9 cc (± 14.5) for 18F-miso and 36.0 cc (± 10.1) for per-treatment 18FDG. In standard plan (66 Gy), the mean dose covering 95% of the PTV (D95%) were 66.5 (± 0.33), 66.1 (± 0.32) and 66.1 (± 0.32) Gy for 18FDG hotspot, 18F-miso and per-treatment 18FDG. In scenario 2, the mean D95% was 72.5 (± 0.25) Gy in 18FDG hotspot versus 67.9 (± 0.49) and 67.9 Gy (± 0.52) in 18F-miso and per-treatment 18FDG, respectively. In scenario 3, the mean D95% was 72.2 (± 0.27) Gy to 18F-miso versus 70.4 (± 0.74) and 69.5Gy (± 0.74) for 18FDG hotspot and per-treatment 18FDG, respectively. In scenario 4, the mean D95% was 73.1 (± 0.3) Gy to 18FDG per-treatment versus 71.9 (± 0.61) and 69.8 (± 0.61) Gy for 18FDG hotspot and 18F-miso, respectively. The dose/volume constraints to OARs were matched in all scenarios.
Conclusion: Escalated doses can be selectively planned in NSCLC target volumes delineated on 18FDG and 18F-miso PET/CT functional images. The most relevant strategy should be investigated in clinical trials.
Trial registration: (RTEP5, NCT01576796 , registered 15 june 2012).
Keywords: 18fluoro-deoxy-D-glucose; 18fluoro-misonidasole; Hypoxia; Lung cancer; Positron emission tomography; Radiotherapy.
Conflict of interest statement
Ethics approval and consent to participate
All data were extracted from one prospective study (NCT01576796). For all patients, we are a consent.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Arriagada R, Le Chevalier T, Quoix E, Ruffie P, de Cremoux H, Douillard JY, et al. ASTRO (American Society for Therapeutic Radiology and Oncology) plenary: effect of chemotherapy on locally advanced non-small cell lung carcinoma: a randomized study of 353 patients. GETCB (Groupe d'Etude et Traitement des cancers Bronchiques), FNCLCC (Féderation Nationale des Centres de Lutte contre le Cancer) and the CEBI trialists. Int J Radiat Oncol Biol Phys. 1991;20(6):1183–1190. doi: 10.1016/0360-3016(91)90226-T. - DOI - PubMed
-
- Bradley JD, Paulus R, Komaki R, Masters G, Blumenschein G. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): a randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015;16(2):187–199. doi: 10.1016/S1470-2045(14)71207-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
