

Neoadjuvant ipilimumab (3 mg/kg or 10 mg/kg) and high dose IFN-α2b in locally/regionally advanced melanoma: safety, efficacy and impact on T-cell repertoire
- PMID: 30352626
- PMCID: PMC6199801
- DOI: 10.1186/s40425-018-0428-5
Neoadjuvant ipilimumab (3 mg/kg or 10 mg/kg) and high dose IFN-α2b in locally/regionally advanced melanoma: safety, efficacy and impact on T-cell repertoire
Abstract
Background: Neoadjuvant immunotherapy utilizing novel combinations has the potential to transform the standard of care for locally/regionally advanced melanoma. We hypothesized that neoadjuvant ipilimumab in combination with high dose IFNα2b (HDI) is safe and associated with durable pathologic complete responses (pCR).
Methods: Patients with locally/regionally advanced melanoma were randomized to ipilimumab 3 or 10 mg/kg × 4 doses bracketing definitive surgery, then every 12 weeks × 4. HDI was given concurrently. We evaluated the safety and efficacy of the combination with ipilimumab 3 or 10 mg/kg. The impact on T-cell fraction and clonality were investigated in tumor and blood.
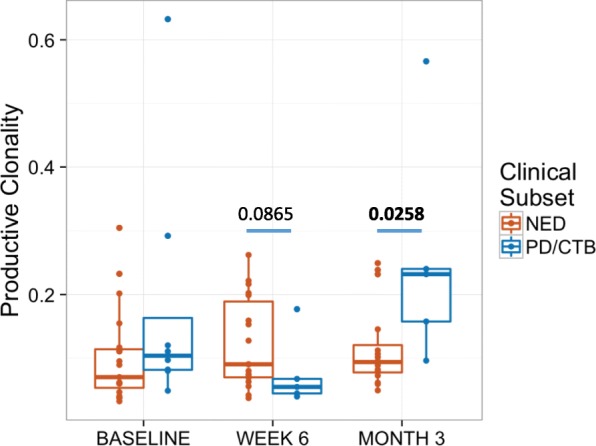
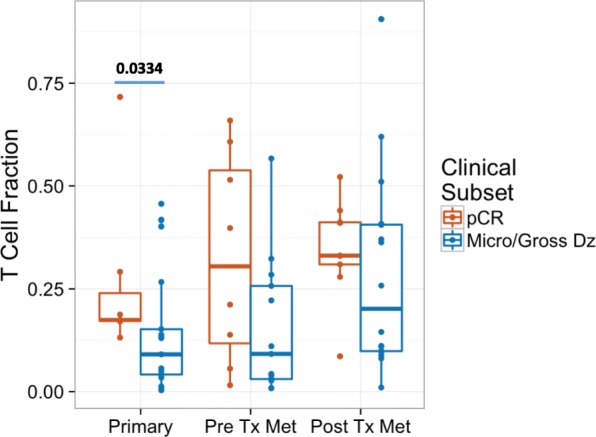
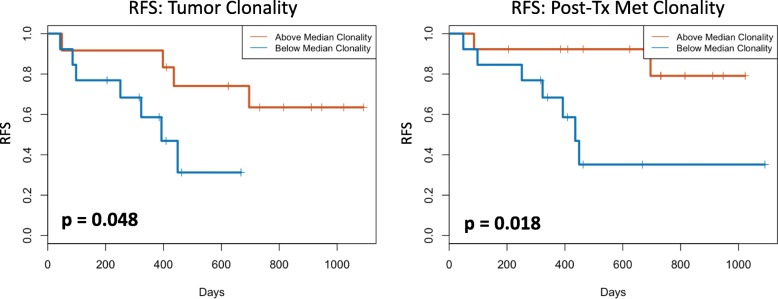
Results: Thirty patients (age 37-76), 15 each at 3 and 10 mg/kg, 18 male and 12 female were treated. Considering immune related adverse events (irAEs) of interest, more grade 3/4 irAEs were seen with ipilimumab 10 mg/kg versus 3 mg/kg (p = 0.042). Among 28 evaluable patients, 11 relapsed, of whom 5 died. Median follow-up for 17 patients who have not relapsed was 32 months. The radiologic preoperative response rate was 36% (95% CI, 21-54); 4 patients at ipilimumab 3 mg/kg and 6 at 10 mg/kg and 2 (at 10 mg/kg) later relapsed. The pCR was 32% (95% CI, 18-51); 5 patients at ipilimumab 3 mg/kg and 4 at 10 mg/kg and one (at 3 mg/kg) had a late relapse. In patients with pCR, T-cell fraction was significantly higher when measured in primary melanoma tumors (p = 0.033). Higher tumor T-cell clonality in primary tumor and more so following neoadjuvant therapy was significantly associated with improved relapse free survival.
Conclusions: Neoadjuvant ipilimumab-HDI was relatively safe and exhibited promising tumor response rates with an associated measurable impact on T-cell fraction and clonality. Most pCRs were durable supporting the value of pCR as a primary endpoint in neoadjuvant immunotherapy trials.
Trial registration: ClinicalTrials.gov, NCT01608594 . Registered 31 May 2012.
Keywords: Anti-CTLA-4; Immunotherapy; Interferon; Ipilimumab; Melanoma.
Conflict of interest statement
Ethics approval and consent to participate
The study was initiated after approval from the institutional review board (IRB) and was conducted in accordance with the Declaration of Helsinki. A University of Pittsburgh IRB approved written informed consent (IRB# PRO12020161) was obtained from all patients.
Consent for publication
Not applicable.
Competing interests
Dr. Tarhini received research grant support Merck, Bristol Myers Squibb and Adaptive Biotechnologies. Dr. Tarhini served as a consultant for Merck, Bristol Myers Squibb, HUYA, Pfizer, Sanofi Genzyme, Novartis, Genentech-Roche, Array Biopharma, NewLink Genetics. John M Kirkwood declared consulting or advisory role to BMS, Merck, Novartis, Roche, Genentech, EMD Serrono, Array Biopharma, Prometheus. Erik C. Yusko and Julie A. Rytlewski are employees or Adaptive Biotechnologies. The rest of the authors declare no potential conflicts of interest relevant to the study.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Romano E, Scordo M, Dusza SW, Coit DG, Chapman PB. Site and timing of first relapse in stage III melanoma patients: implications for follow-up guidelines. Journal of clinical oncology : official journal of the. Proc Am Soc Clin Oncol. 2010;28(18):3042–3047. doi: 10.1200/JCO.2009.26.2063. - DOI - PMC - PubMed
-
- Balch CM, Soong SJ, Smith T, Ross MI, Urist MM, Karakousis CP, et al. Long-term results of a prospective surgical trial comparing 2 cm vs. 4 cm excision margins for 740 patients with 1-4 mm melanomas. Ann Surg Oncol. 2001;8(2):101–108. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical