

Urogenital schistosomiasis elimination in Zanzibar: accuracy of urine filtration and haematuria reagent strips for diagnosing light intensity Schistosoma haematobium infections
- PMID: 30352631
- PMCID: PMC6199745
- DOI: 10.1186/s13071-018-3136-6
Urogenital schistosomiasis elimination in Zanzibar: accuracy of urine filtration and haematuria reagent strips for diagnosing light intensity Schistosoma haematobium infections
Erratum in
-
Correction to: Urogenital schistosomiasis elimination in Zanzibar: accuracy of urine filtration and haematuria reagent strips for diagnosing light intensity Schistosoma haematobium infections.Parasit Vectors. 2019 Mar 28;12(1):149. doi: 10.1186/s13071-019-3397-8. Parasit Vectors. 2019. PMID: 30922376 Free PMC article.
Abstract
Background: Urine filtration and microhaematuria reagent strips are basic standard diagnostic methods to detect urogenital schistosomiasis. We assessed their accuracy for the diagnosis of light intensity infections with Schistosoma haematobium as they occur in individuals living in Zanzibar, an area targeted for interruption of transmission.
Methods: Urine samples were collected from children and adults in surveys conducted annually in Zanzibar from 2013 through 2016 and examined with the urine filtration method to count S. haematobium eggs and with the reagent strip test (Hemastix) to detect microhaematuria as a proxy for infection. Ten percent of the urine filtration slides were read twice. Sensitivity was calculated for reagent strips, stratified by egg counts reflecting light intensity sub-groups, and kappa statistics for the agreement of urine filtration readings.
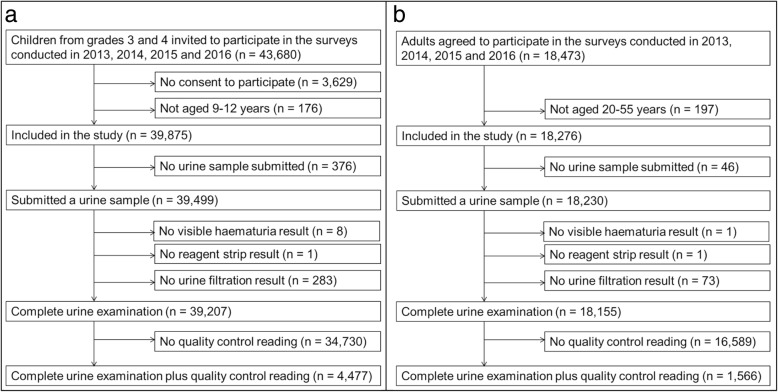
Results: Among the 39,207 and 18,155 urine samples examined from children and adults, respectively, 5.4% and 2.7% were S. haematobium egg-positive. A third (34.7%) and almost half (46.7%) of the egg-positive samples from children and adults, respectively, had ultra-low counts defined as 1-5 eggs per 10 ml urine. Sensitivity of the reagent strips increased significantly for each unit log10 egg count per 10 ml urine in children (odds ratio, OR: 4.7; 95% confidence interval, CI: 4.0-5.7; P < 0.0001) and adults (OR: 2.6; 95% CI: 1.9-3.7, P < 0.0001). Sensitivity for diagnosing ultra-light intensity infections was very low in children (50.1%; 95% CI: 46.5-53.8%) and adults (58.7%; 95% CI: 51.9-65.2%). Among the 4477 and 1566 urine filtration slides read twice from children and adults, most were correctly identified as negative or positive (kappa = 0.84 for children and kappa = 0.81 for adults). However, 294 and 75 slides had discrepant results and were positive in only one of the two readings. The majority of these discrepant slides (76.9% of children and 84.0% of adults) had counts of 1-5 eggs per 10 ml urine.
Conclusions: We found that many individuals infected with S. haematobium in Zanzibar excrete > 5 eggs per 10 ml urine. These ultra-light infections impose a major challenge for accurate diagnosis. Next-generation diagnostic tools to be used in settings where interruption of transmission is the goal should reliably detect infections with ≤ 5 eggs per 10 ml urine.
Trial registration: ISRCTN, ISRCTN48837681 . Registered 05 September 2012 - Retrospectively registered.
Keywords: Control; Diagnosis; Elimination; Macrohaematuria; Microhaematuria; Reagent strip; Schistosoma haematobium; Surveillance; Urine filtration; Urogenital schistosomiasis; Zanzibar.
Conflict of interest statement
Ethics approval and consent to participate
Our study protocol was approved by the Zanzibar Medical Research Ethics Committee (ZAMREC) in Zanzibar, United Republic of Tanzania (reference no. ZAMREC 0003/Sept/011), the Ethics Committee of Basel, Switzerland (reference no. EKBB 236/11), and the Institutional Review Board of the University of Georgia in the USA (project no. 2012-10138-0) [16]. The study is registered with the International Standard Randomized Controlled Trial Number register (ISRCTN48837681). All children and adults invited to participate in the study received a participant information sheet and a consent sheet. The study was explained in lay terms to the children in school and to the adults in the communities using the local language Kiswahili. Only individuals, who submitted a written informed consent for their participation, were included in the study. In the case of children, parents or their legal guardians were asked to provide their written consent for the child’s participation. All study participants were offered praziquantel (40 mg/kg) against schistosomiasis and albendazole (400 mg) against soil-transmitted helminthiasis free of charge
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- WHO . WHA65.21. Elimination of schistosomiasis. Sixty-fifth World Health Assembly Geneva 21–26 May 2012 Resolutions, decisions and annexes. Geneva: World Health Organization; 2012. pp. 36–37.
-
- WHO . Schistosomiasis: progress report 2001–2011 and strategic plan 2012–2020. Geneva: World Health Organization; 2013. pp. 1–80.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
