

Pneumococcal carriage in households in Karonga District, Malawi, before and after introduction of 13-valent pneumococcal conjugate vaccination
- PMID: 30352744
- PMCID: PMC6238076
- DOI: 10.1016/j.vaccine.2018.10.021
Pneumococcal carriage in households in Karonga District, Malawi, before and after introduction of 13-valent pneumococcal conjugate vaccination
Abstract
Background: Thirteen-valent pneumococcal conjugate vaccine (PCV13) was introduced in Malawi in November 2011 and is offered to infants at 6, 10 and 14 weeks of age as part of routine immunisation. PCV13 is expected to reduce vaccine type (VT) nasopharyngeal carriage, leading to reduced transmission and herd protection.
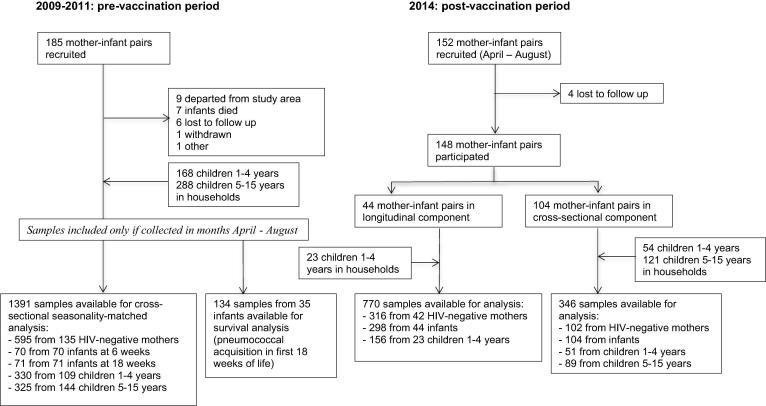
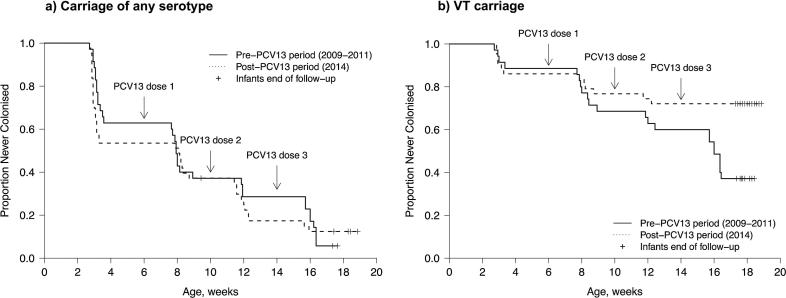
Methods: We compared pneumococcal carriage in rural Karonga District, Malawi, pre-vaccine in 2009-2011 and post-vaccine in 2014 using a combination of cross-sectional and longitudinal analyses. Nasopharyngeal swabs were collected from a cohort of mother-infant pairs and household members <16 years. Pneumococci from 2009 to 2011 were serogrouped using latex agglutination and serotyped by Quellung reaction. In 2014, latex agglutination was used for both steps. Carriage prevalence ratios using prevalence data from before and after vaccine introduction were calculated by log-binomial regression, adjusted for age, seasonality and household composition. Participating infants in 2014 received PCV13 as part of routine immunisation.
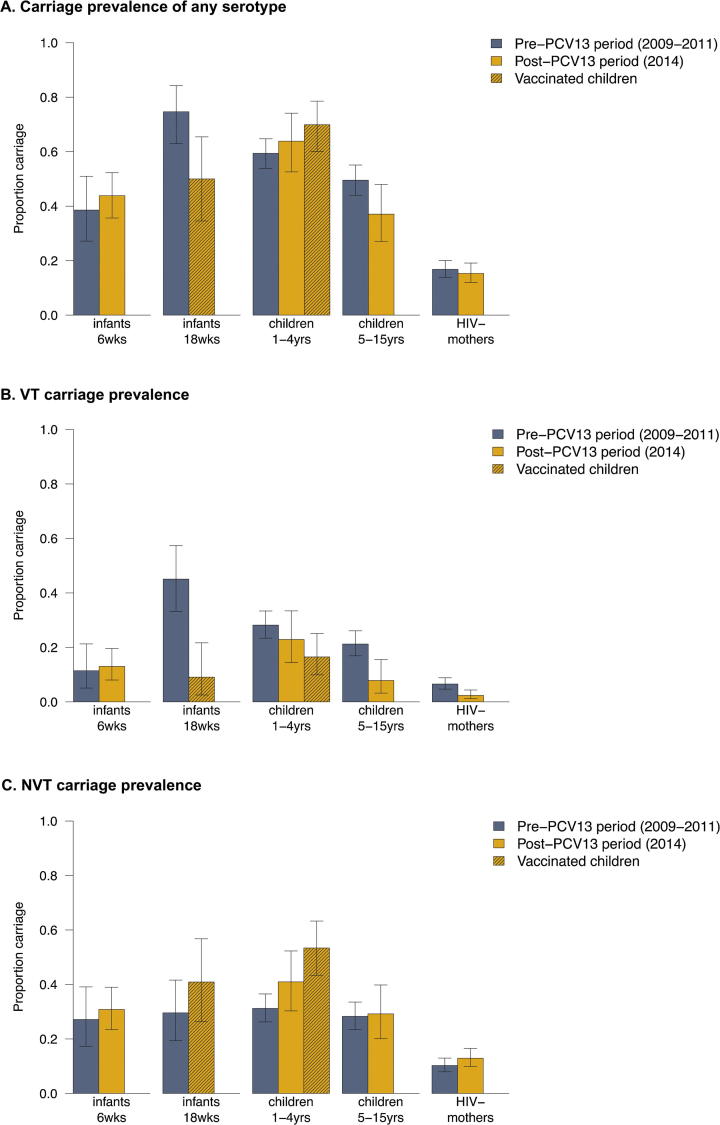
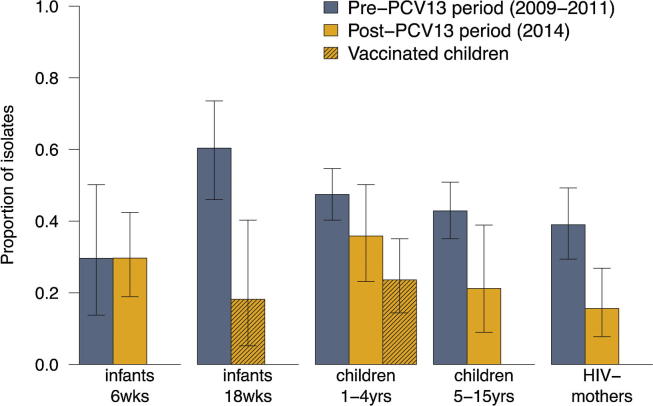
Results: VT carriage prior to PCV-13 introduction was 11.4%, 45.1%, 28.2%, 21.2% and 6.6% for 6-week old infants, 18-week old infants, children 1-4 years, children 5-15 years and mothers, respectively. After vaccine introduction, VT carriage decreased among vaccinated 18-week old infants (adjusted prevalence ratio 0.24 (95%CI 0.08-0.75)), vaccinated children 1-4 years (0.54 (0.33-0.88)), unvaccinated children 5-15 years (0.37 (0.17-0.78)) and mothers (0.34 (0.15-0.79)). No decrease in VT carriage was observed for 6-week old infants too young to be vaccinated (1.07 (0.38-3.02)) and PCV-13 ineligible children 1-4 years (0.84 (0.53-1.33)). Non-VT carriage increased only among vaccinated children 1-4 years (1.58 (1.21-2.06)).
Conclusions: There is evidence of reduced VT pneumococcal carriage three years after vaccine introduction in this rural Malawian population with good vaccine coverage using a 3 + 0 schedule. However carriage was sustained among 6-week-old infants and PCV13 ineligible 1-4 year olds, and there was some indication of serotype replacement in vaccinated 1-4 year olds.
Keywords: Africa; Carriage; Cohort studies; Infant; Pneumococcal conjugate vaccine; Streptococcus pneumoniae.
Copyright © 2018 Univerity of Liverpool. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Bogaert D., De Groot R., Hermans P.W. Streptococcus pneumoniae colonisation: the key to pneumococcal disease. Lancet Infect Dis. 2004;4(3):144–154. - PubMed
-
- Granat S.M., Mia Z., Ollgren J. Longitudinal study on pneumococcal carriage during the first year of life in Bangladesh. Pediatr Infect Dis J. 2007;26(4):319–324. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
