

Sensory attenuation in Parkinson's disease is related to disease severity and dopamine dose
- PMID: 30353104
- PMCID: PMC6199336
- DOI: 10.1038/s41598-018-33678-3
Sensory attenuation in Parkinson's disease is related to disease severity and dopamine dose
Erratum in
-
Publisher Correction: Sensory attenuation in Parkinson's disease is related to disease severity and dopamine dose.Sci Rep. 2018 Nov 22;8(1):17429. doi: 10.1038/s41598-018-35439-8. Sci Rep. 2018. PMID: 30467360 Free PMC article.
Abstract
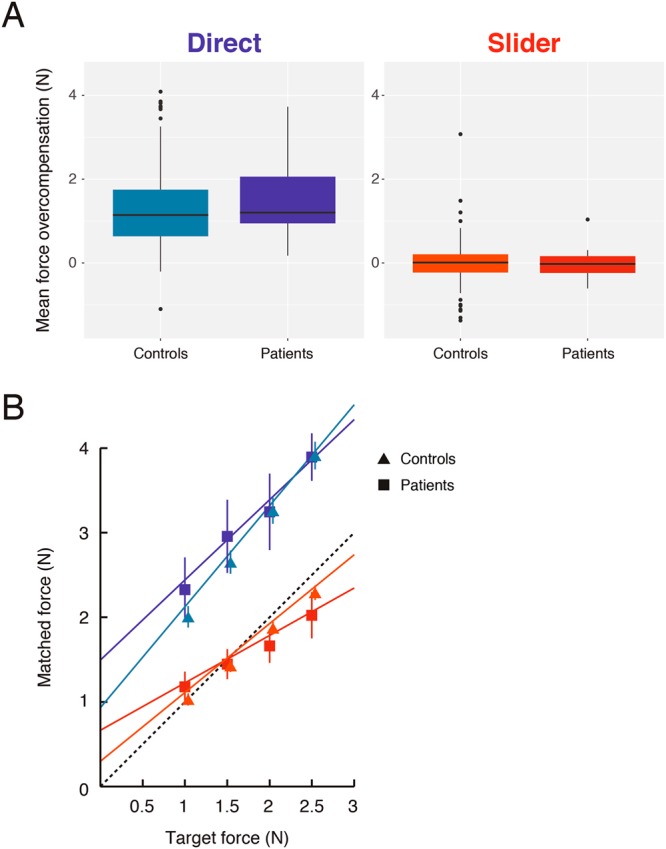
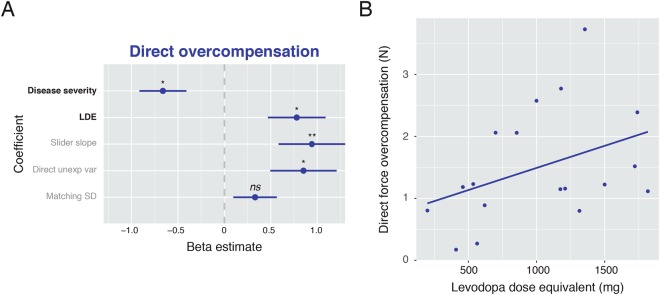
Abnormal initiation and control of voluntary movements are among the principal manifestations of Parkinson's disease (PD). However, the processes underlying these abnormalities and their potential remediation by dopamine treatment remain poorly understood. Normally, movements depend on the integration of sensory information with the predicted consequences of action. This integration leads to a suppression in the intensity of predicted sensations, reflected in a 'sensory attenuation'. We examined this integration process and its relation to dopamine in PD, by measuring sensory attenuation. Patients with idiopathic PD (n = 18) and population-derived controls (n = 175) matched a set of target forces applied to their left index finger by a torque motor. To match the force, participants either pressed with their right index finger ('Direct' condition) or moved a knob that controlled a motor through a linear potentiometer ('Slider' condition). We found that despite changes in sensitivity to different forces, overall sensory attenuation did not differ between medicated PD patients and controls. Importantly, the degree of attenuation was negatively related to PD motor severity but positively related to individual patient dopamine dose, as measured by levodopa dose equivalent. The results suggest that dopamine could regulate the integration of sensorimotor prediction with sensory information to facilitate the control of voluntary movements.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
