

Introduction to contrast-enhanced ultrasound of the brain in neonates and infants: current understanding and future potential
- PMID: 30353273
- PMCID: PMC6604800
- DOI: 10.1007/s00247-018-4270-1
Introduction to contrast-enhanced ultrasound of the brain in neonates and infants: current understanding and future potential
Abstract
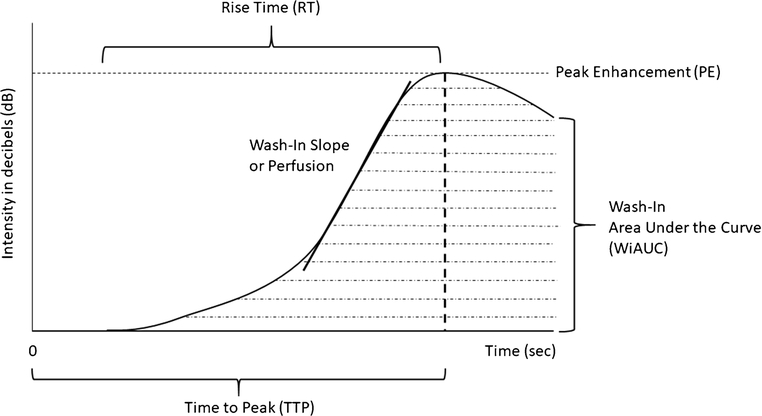
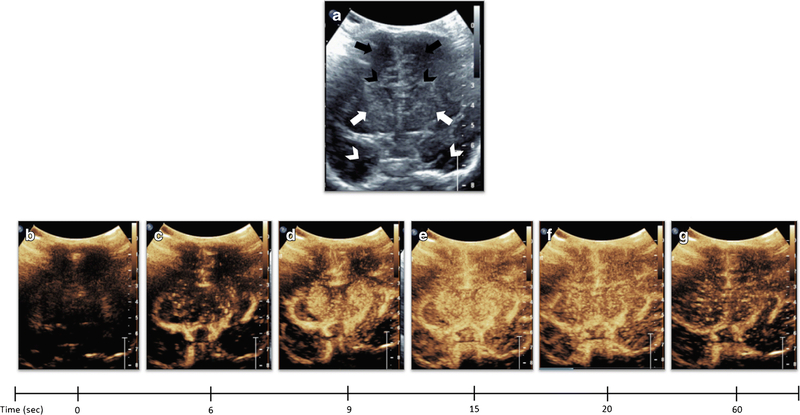
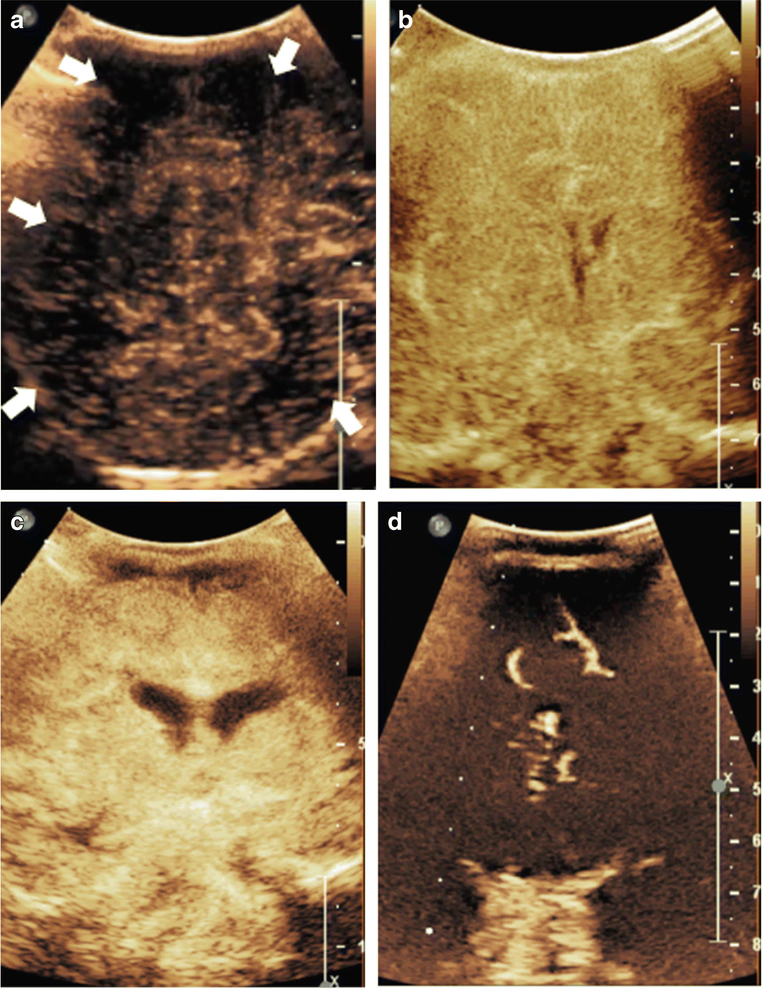
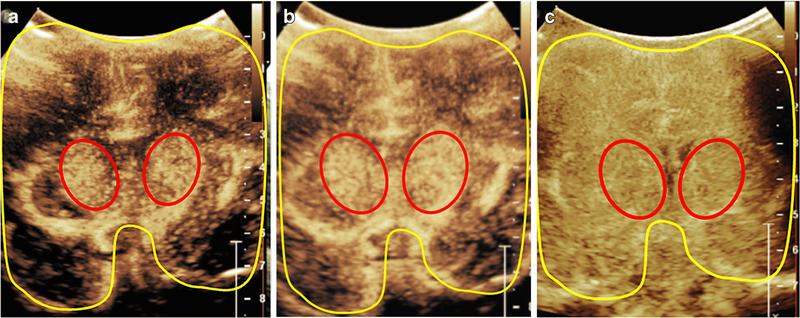
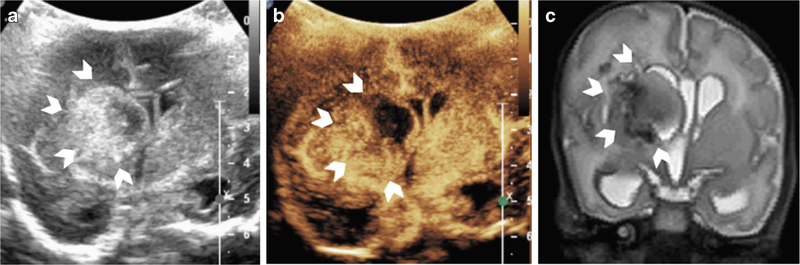
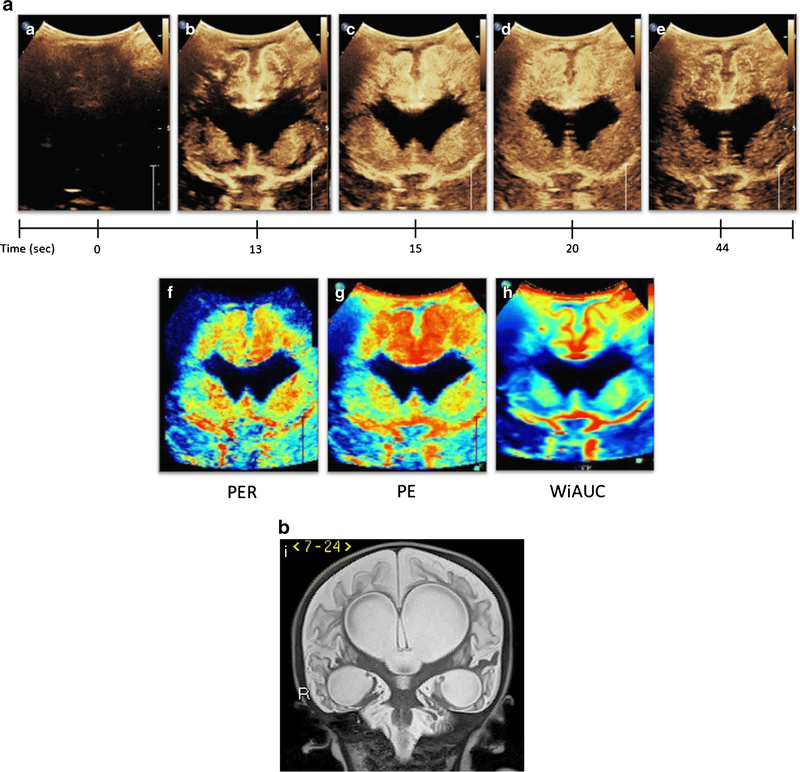
Contrast-enhanced ultrasound (CEUS) is a valuable bedside imaging technique that enables both qualitative and quantitative assessment of cerebral perfusion. In neonates and infants whose fontanelles remain open, the technique is particularly useful as it delineates cerebral pathology with high soft-tissue contrast. The technique has the potential to be a valuable alternative to computed tomography (CT) or magnetic resonance imaging (MRI) in critically ill neonates and infants in need of bedside imaging. While further studies are needed to validate the technique, preliminary data in this regard appear promising. This review introduces the current understanding and future potential of brain CEUS.
Keywords: Brain; Clinical protocol; Contrast-enhanced ultrasound; Neonate; Perfusion; Ultrasound.
Figures
References
-
- Hwang M, de Jong RM, Herman S et al. (2016) Novel Contrast Ultrasound Evaluation in Neonatal Hypoxic Ischemic Injury: Case Series and Future Directions. J Ultrasound Med 36:2379–2386 - PubMed
-
- Hwang M, Riggs BJ, Katz J et al. (2018) Advanced Pediatric Neurosonography Techniques: Contrast-Enhanced Ultrasonography, Elastography, and Beyond. J Neuroimaging 28:150–157. - PubMed
-
- Hwang M, Sridharan A, Darge K et al. (2018) Novel Quantitative Contrast-Enhanced Ultrasound Detection of Hypoxic Ischemic Injury in Neonates and Infants: Pilot Study I. - PubMed
-
- Ilves P, Lintrop M, Talvik I et al. (2009) Low cerebral blood flow velocity and head circumference in infants with severe hypoxic ischemic encephalopathy and poor outcome. Acta Paediatr 98:459–465 - PubMed
-
- Okereafor A, Allsop J, Counsell SJ et al. (2008) Patterns of brain injury in neonates exposed to perinatal sentinel events. Pediatrics 121:906–914 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
