

Association of social deprivation with 1-year outcome of ICU survivors: results from the FROG-ICU study
- PMID: 30353380
- PMCID: PMC7095041
- DOI: 10.1007/s00134-018-5412-5
Association of social deprivation with 1-year outcome of ICU survivors: results from the FROG-ICU study
Abstract
Purpose: Intensive care unit survivors suffer from prolonged impairment, reduced quality of life, and higher mortality rates after discharge compared to the general population. Socioeconomic status may play a partial but important role in mortality and recovery. Therefore, the detection of factors that are responsible for poor long-term outcomes would be beneficial in designing targeted interventions for at-risk populations.
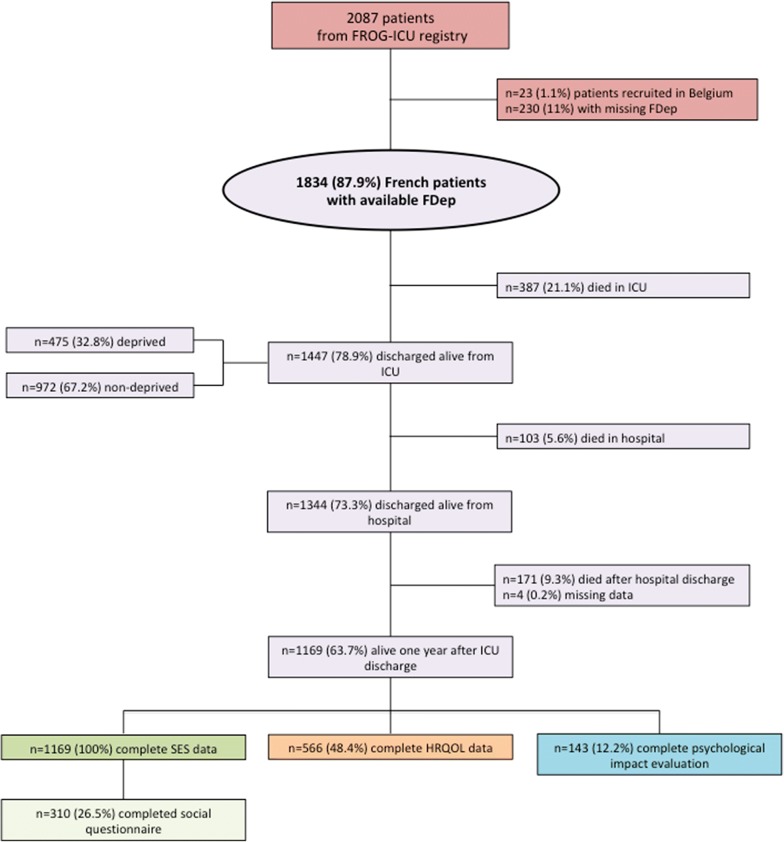
Methods: For an endpoint analysis, 1834 intensive care unit patients with known French Deprivation Index (FDep) scores were included from the French and euRopean Outcome reGistry in Intensive Care Units (FROG-ICU) study, which was a prospective, observational, multicenter cohort study performed in 20 French intensive care units in 13 different hospitals. Socioeconomic status was defined by using the FDep score [represented as quintiles when referring to the general French population, as quintiles when referring to the FROG-ICU cohort, or as dichotomized data (which was defined as a FDep ≤ 0 for nondeprived patients)] and by using a detailed social questionnaire that was completed 3 months after discharge. The primary outcome included an all-cause, 1-year mortality after ICU discharge when regarding socioeconomic status. The secondary outcomes included both ICU and hospital lengths of stay, both short- and medium-term mortality, and the quality of life, as assessed during the 1-year follow-up by using the Medical Outcome Survey Short Form-36 (SF-36). The Revised Impact of Event Scale (IES-R) was used to evaluate the symptoms of post-traumatic stress disorder, and the Hospital Anxiety and Depression Scale (HADS) was used to screen for anxiety and depression.
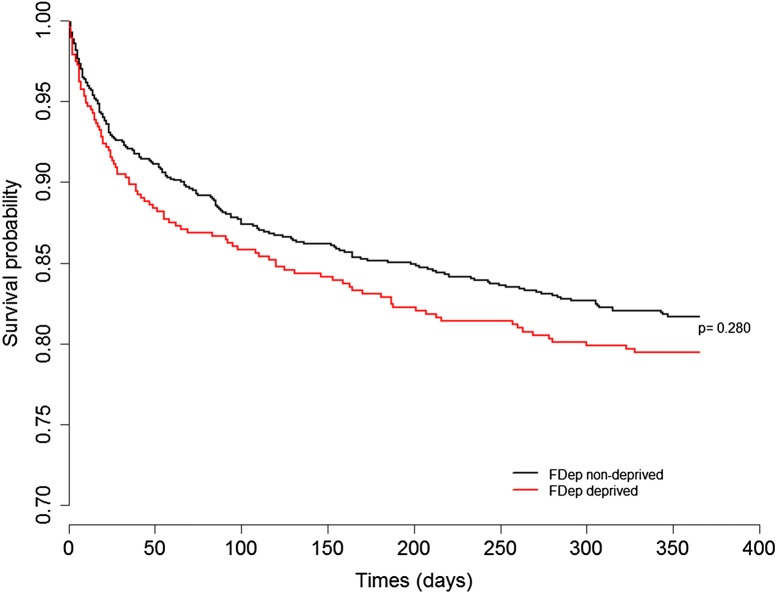
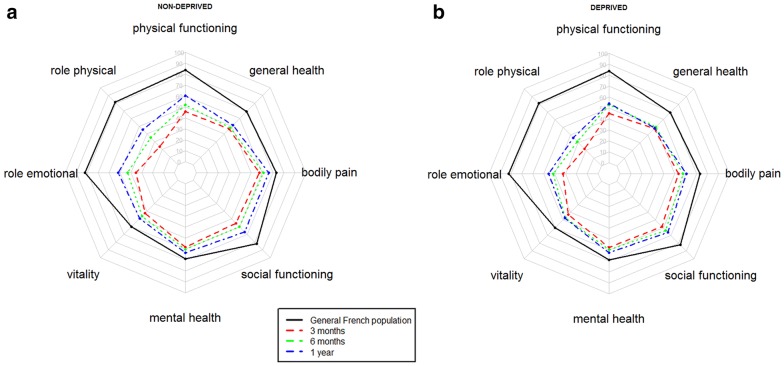
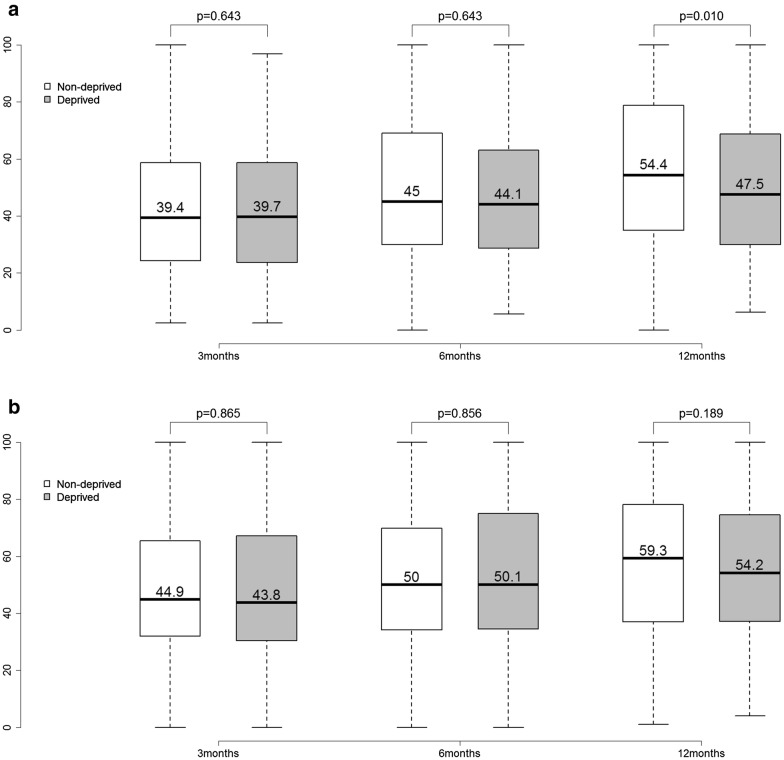
Results: Of the 1447 patients who were discharged alive from the ICU, 19.2% died over the following year. No association was found between 1-year mortality and socioeconomic status, regardless of whether this association was analyzed in quintiles (p = 0.911 in the quintiles of the general French population; p = 0.589 in the quintiles of the FROG-ICU cohort itself) or as dichotomized data [nondeprived (n = 177; 1-year mortality of 18.2%) versus deprived (n = 97; 1-year mortality of 20.5%; p = 0.304)]. Moreover, no differences were found between the nondeprived and the deprived patients in the ICU and hospital lengths of stay, ICU mortalities, in-hospital mortalities, or 28-day mortalities. The SF-36 was below the score for the normal French population throughout the follow-up period. Socially deprived patients showed significantly lower median scores in the physical function subscale [55, interquartile range (IQR) (28.8-80) vs. 65, IQR (35-90); p = 0.014], the physical role subscale [25, IQR (0-75) vs. 33.3, IQR (0-100); p = 0.022], and the overall physical component scale [47.5, IQR (30-68.8) vs. 54.4, IQR (35-78.8); p = 0.010]. Up to 31.6% of survivors presented symptoms that indicated post-traumatic stress disorder, and up to 31.5% of survivors reported clinically meaningful symptoms of anxiety or depression.
Conclusions: A lower socioeconomic status was associated with lower self-reported physical component scores in the nondeprived patients. Psychiatric symptoms are frequently reported after an ICU stay, and subsequent interventions should target those fields.
Trial registration: ClinicalTrials.gov NCT01367093; registered on June 6, 2011.
Keywords: FDep; HADS; IES-R; Post-traumatic stress disorder; SF-36; Socioeconomic status.
Conflict of interest statement
None of the authors of this paper has a financial or personal relationship with other persons or organizations that could inappropriately influence or bias the content of the paper. Etienne Gayat received a research grant from sphingotec and consultancy fees from Magnisense and Roche Diagnostics. Alexandre Mebazaa received speaker’s honoraria from Abbott, Novartis, Orion, Roche, and Servier and a fee as a member of the advisory board and/or steering committee from Cardiorentis, Adrenomed, MyCartis, Neurotronik, and sphingotec. Martin Siegemund received speaker’s honoraria from Fresenius, Orion Pharma, and SwissOrpha and a research grant from Octapharma. The original FROG-ICU study was supported by grants from Assistance Publique-Hôpitaux de Paris (AOR01004) and from Société Française d’Anesthésie–Réanimation.
Figures
References
-
- Bienvenu OJ, Friedman LA, Colantuoni E, Dinglas VD, Sepulveda KA, Mendez-Tellez P, Shanholz C, Pronovost PJ, Needham DM. Psychiatric symptoms after acute respiratory distress syndrome: a 5-year longitudinal study. Intensive Care Med. 2018;44:38–47. doi: 10.1007/s00134-017-5009-4. - DOI - PMC - PubMed
-
- Graf JJ, Uwe J. Der post-intensivpatient. Langzeitüberleben und lebensqualität nach intensivtherapie. Intensivmed Notfallmedizin. 2003;40:184–194. doi: 10.1007/s00390-003-0347-6. - DOI
