

Immunosuppression and HIV Viremia Associated with More Atherogenic Lipid Profile in Older People with HIV
- PMID: 30353737
- PMCID: PMC6343189
- DOI: 10.1089/AID.2018.0145
Immunosuppression and HIV Viremia Associated with More Atherogenic Lipid Profile in Older People with HIV
Abstract
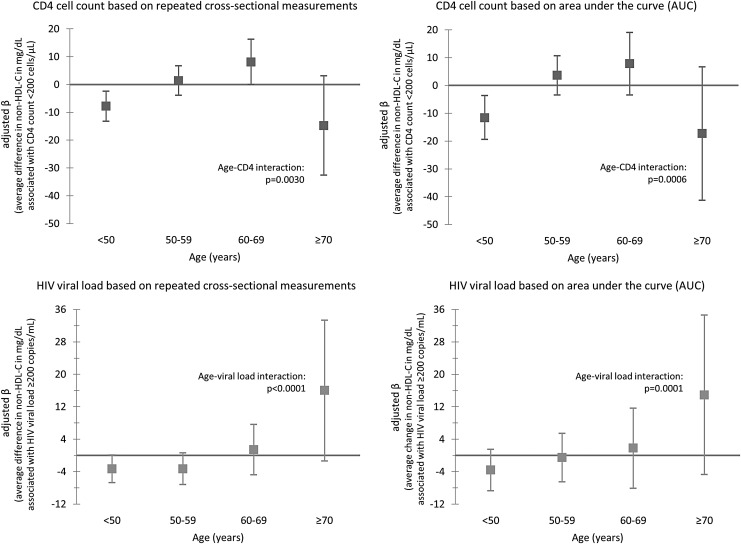
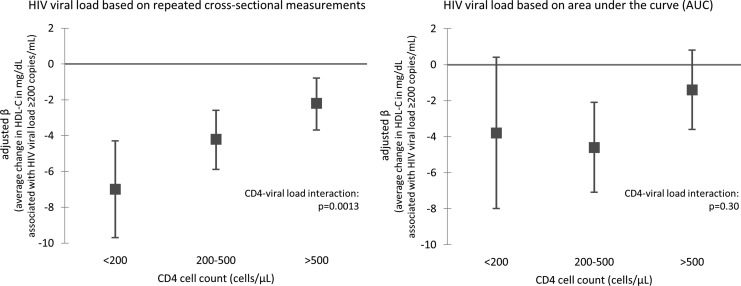
To explore reasons for the disproportionate metabolic and cardiovascular disease burdens among older HIV-infected persons, we investigated whether associations of CD4 count and HIV viral load (VL) with non-high-density lipoprotein cholesterol (non-HDL-C) and high-density lipoprotein cholesterol [HDL-C] differed by age. Longitudinal clinical and laboratory data were collected between 2011 and 2016 for HIV-infected outpatients in the DC Cohort study. Using data for patients aged ≥21 years with ≥1 cholesterol result and contemporaneous CD4/VL results, we created multivariable linear regression models with generalized estimating equations. Among 3,912 patients, the median age was 50 years, 78% were male, 76% were non-Hispanic black, 93% were using antiretroviral therapy, 8% had a CD4 count <200 cells/μL, and 18% had an HIV VL ≥200 copies/mL. Overall, CD4 count <200 (vs. >500) cells/μL and VL ≥200 copies/mL were associated with lower non-HDL-C concentrations (p < .01), but associations were more positive with increasing age (CD4-age/VL-age interactions, p < .01). CD4 count <200 cells/μL was associated with lower non-HDL-C among patients aged <50 years [β = -7.8 mg/dL (95% confidence interval, CI: -13.2 to -2.4)] but higher non-HDL-C among patients aged 60-69 years [β = +8.1 mg/dL (95% CI: 0.02-16.2)]. VL ≥200 copies/mL was associated with lower non-HDL-C among patients aged <50 years [β = -3.3 mg/dL (95% CI: -6.7 to 0.1)] but higher non-HDL-C among patients aged ≥70 years [β = +16.0 mg/dL (95% CI: -1.4 to 33.3)], although precision was reduced in age-stratified analyses. Although no age differences were detected for HDL-C, VL ≥200 copies/mL was more strongly associated with lower HDL-C concentrations when CD4 count was <200 cells/μL [β = -7.0 mg/dL (95% CI: -9.7 to -4.3)] versus 200-500 cells/μL [β = -4.2 (95% CI: -5.9 to -2.6)] or >500 cells/μL [β = -2.2 (95% CI: -3.7 to -0.8)] (CD4-VL interaction, p < .01). We detected a novel age-modified relationship between immunosuppression and viremia and atherogenic cholesterol patterns. These findings may contribute to our understanding of the high risk of dyslipidemia observed among persons aging with HIV.
Keywords: CD4 cell count; HIV; age; cholesterol; viral load.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Guaraldi G, Orlando G, Zona S, et al. : Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin Infect Dis 2011;53:1120–1126 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
