

Carbamazepine versus phenobarbitone monotherapy for epilepsy: an individual participant data review
- PMID: 30353945
- PMCID: PMC6517155
- DOI: 10.1002/14651858.CD001904.pub4
Carbamazepine versus phenobarbitone monotherapy for epilepsy: an individual participant data review
Abstract
Background: This is an updated version of the Cochrane Review previously published in 2016. This review is one in a series of Cochrane Reviews investigating pair-wise monotherapy comparisons.Epilepsy is a common neurological condition in which abnormal electrical discharges from the brain cause recurrent unprovoked seizures. It is believed that with effective drug treatment, up to 70% of individuals with active epilepsy have the potential to become seizure-free and go into long-term remission shortly after starting drug therapy with a single antiepileptic drug in monotherapy.Worldwide, carbamazepine and phenobarbitone are commonly used broad-spectrum antiepileptic drugs, suitable for most epileptic seizure types. Carbamazepine is a current first-line treatment for focal onset seizures, and is used in the USA and Europe. Phenobarbitone is no longer considered a first-line treatment because of concerns over associated adverse events, particularly documented behavioural adverse events in children treated with the drug. However, phenobarbitone is still commonly used in low- and middle-income countries because of its low cost. No consistent differences in efficacy have been found between carbamazepine and phenobarbitone in individual trials; however, the confidence intervals generated by these trials are wide, and therefore, synthesising the data of the individual trials may show differences in efficacy.
Objectives: To review the time to treatment failure, remission and first seizure with carbamazepine compared with phenobarbitone when used as monotherapy in people with focal onset seizures (simple or complex focal and secondarily generalised), or generalised onset tonic-clonic seizures (with or without other generalised seizure types).
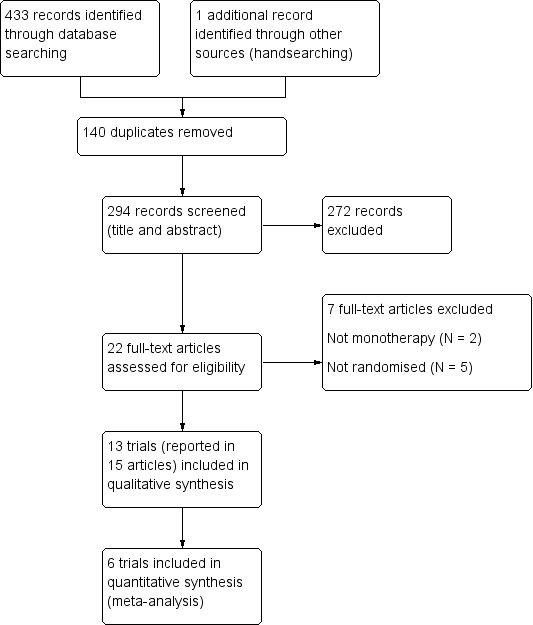
Search methods: For the latest update, we searched the following databases on 24 May 2018: the Cochrane Register of Studies (CRS Web), which includes Cochrane Epilepsy's Specialized Register and CENTRAL; MEDLINE; the US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov); and the World Health Organization International Clinical Trials Registry Platform (ICTRP). We handsearched relevant journals and contacted pharmaceutical companies, original trial investigators, and experts in the field.
Selection criteria: Randomised controlled trials comparing monotherapy with either carbamazepine or phenobarbitone in children or adults with focal onset seizures or generalised onset tonic-clonic seizures.
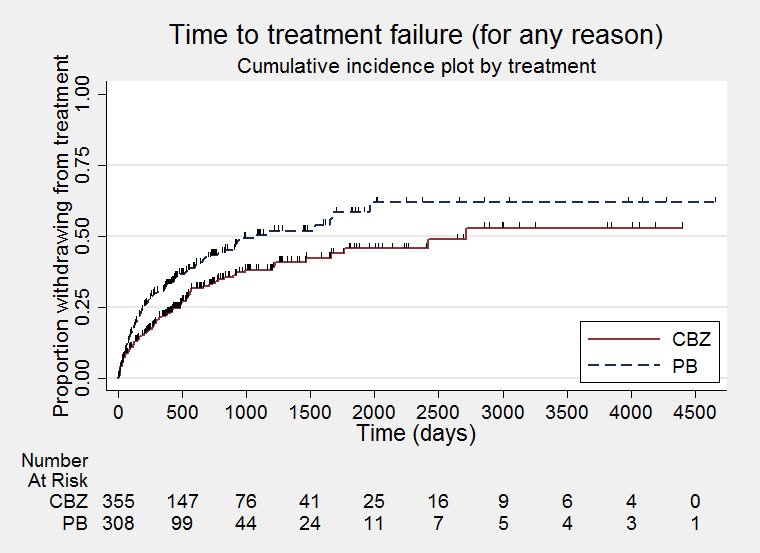
Data collection and analysis: This was an individual participant data (IPD), review. Our primary outcome was time to treatment failure. Our secondary outcomes were time to first seizure post-randomisation, time to six-month remission, time to 12-month remission, and incidence of adverse events. We used Cox proportional hazards regression models to obtain trial-specific estimates of hazard ratios (HRs), with 95% confidence intervals (CIs), using the generic inverse variance method to obtain the overall pooled HR and 95% CI.
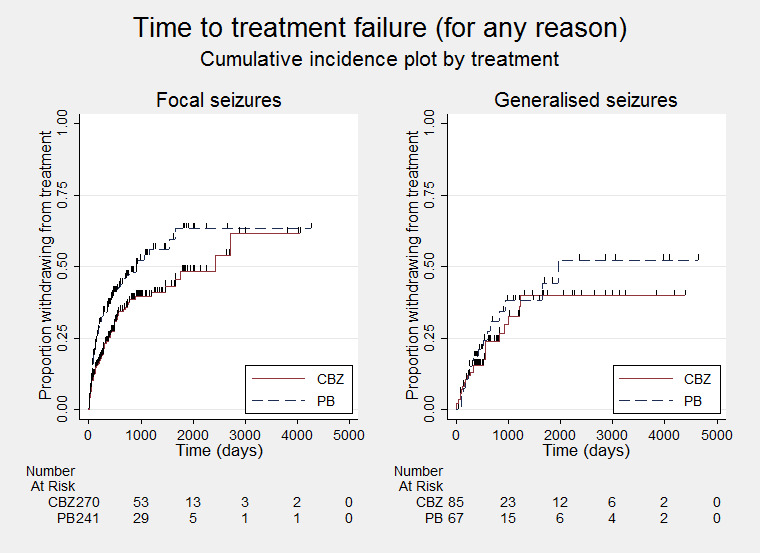
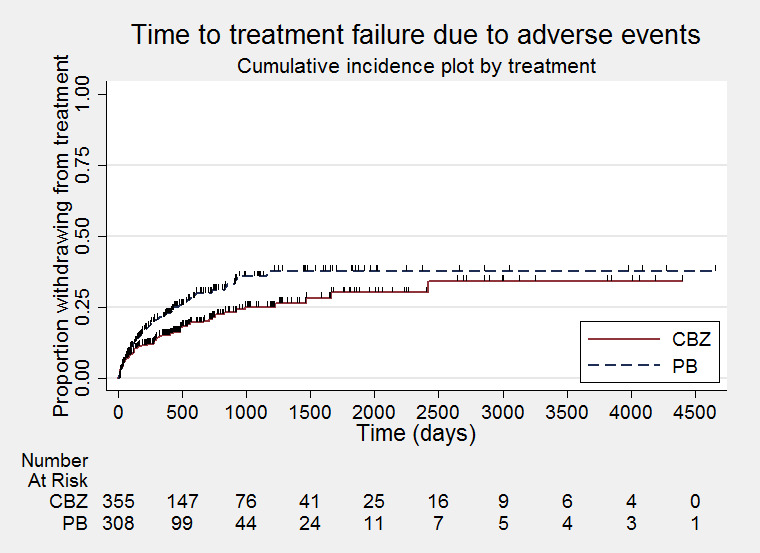
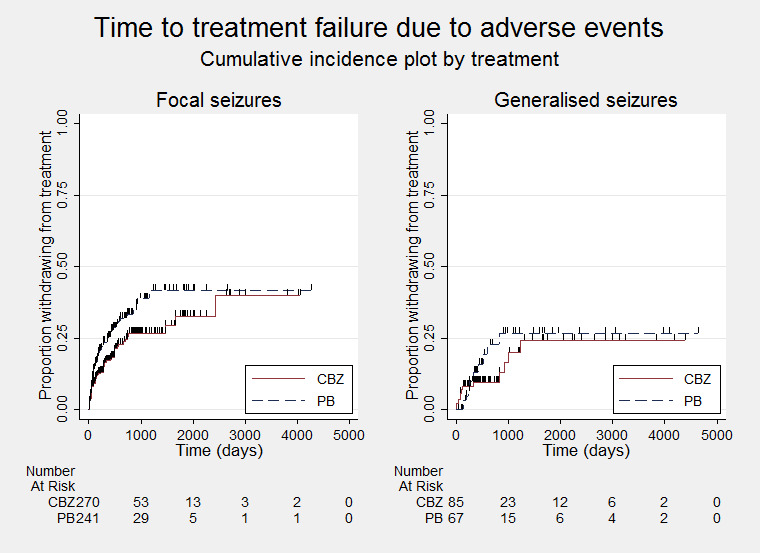
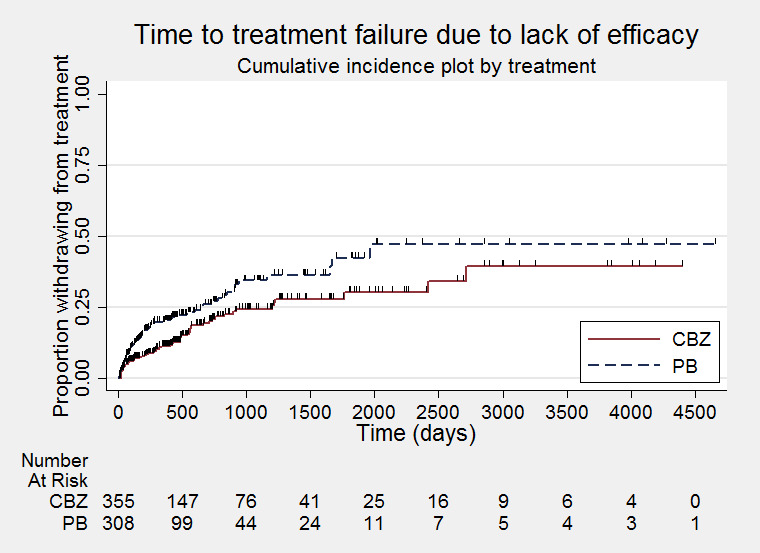
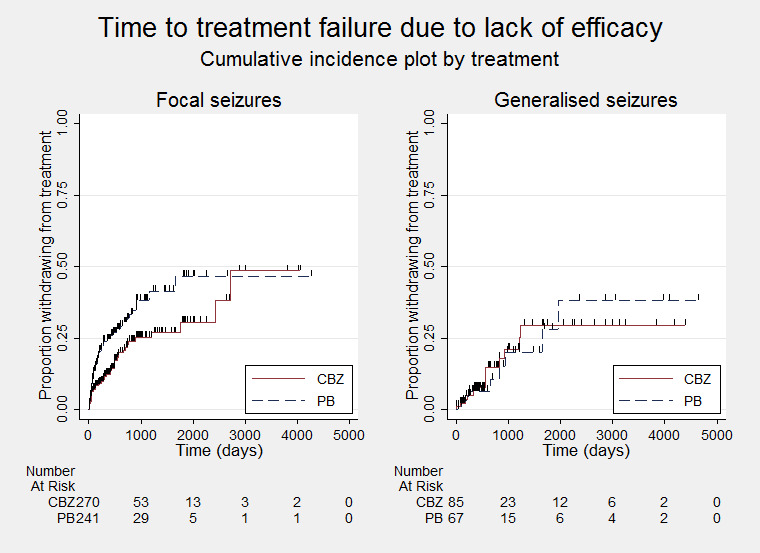
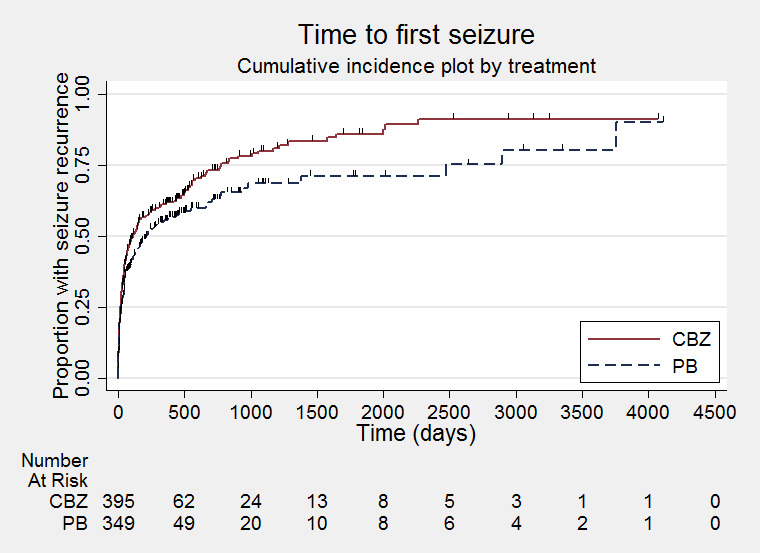
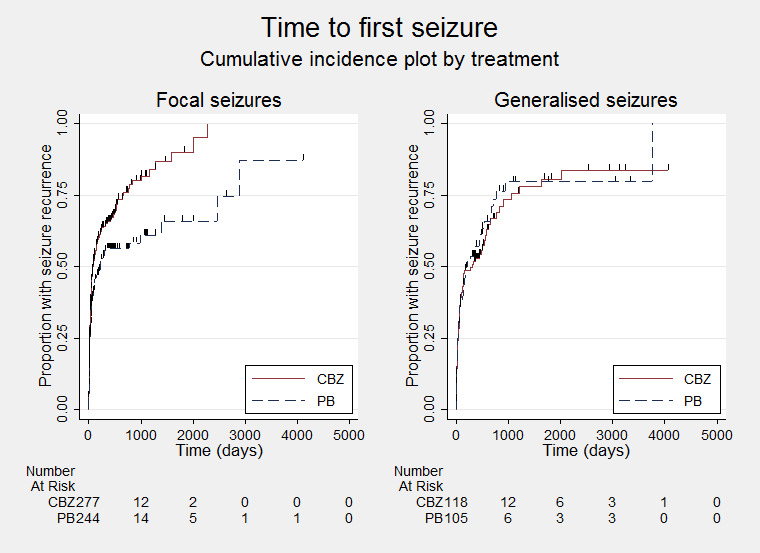
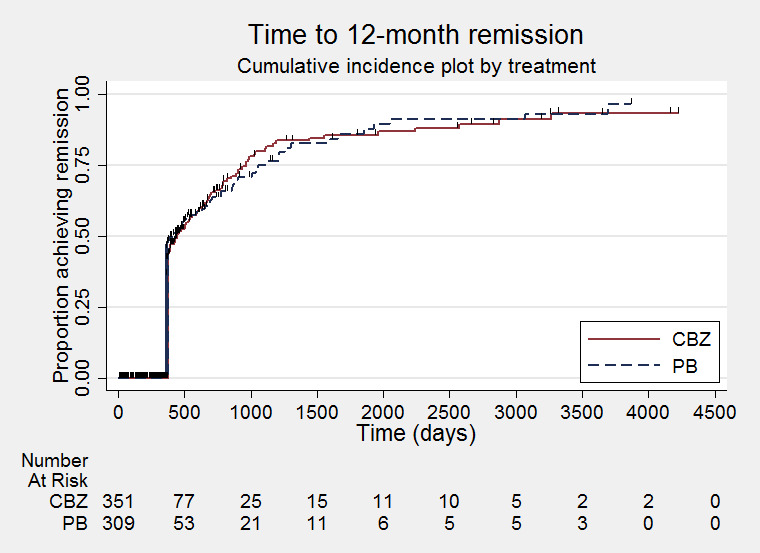
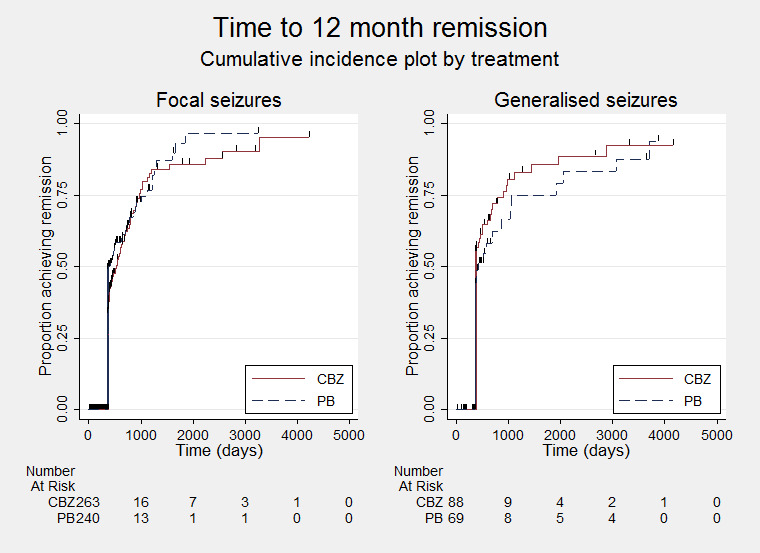
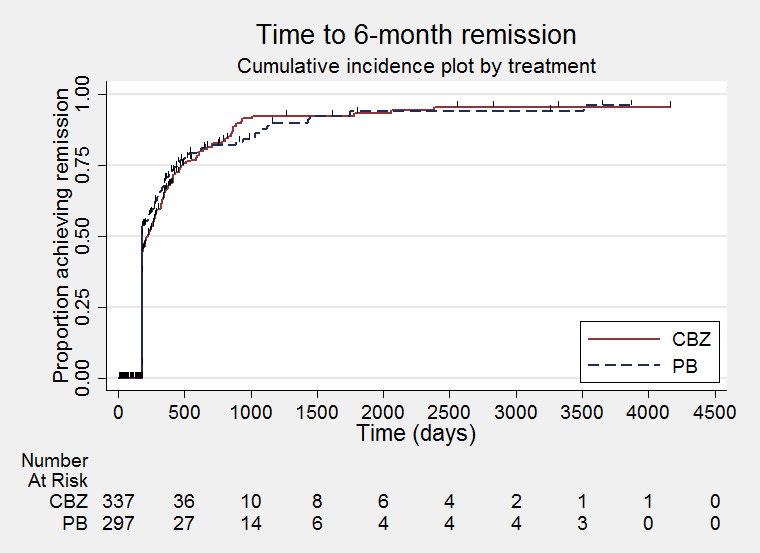
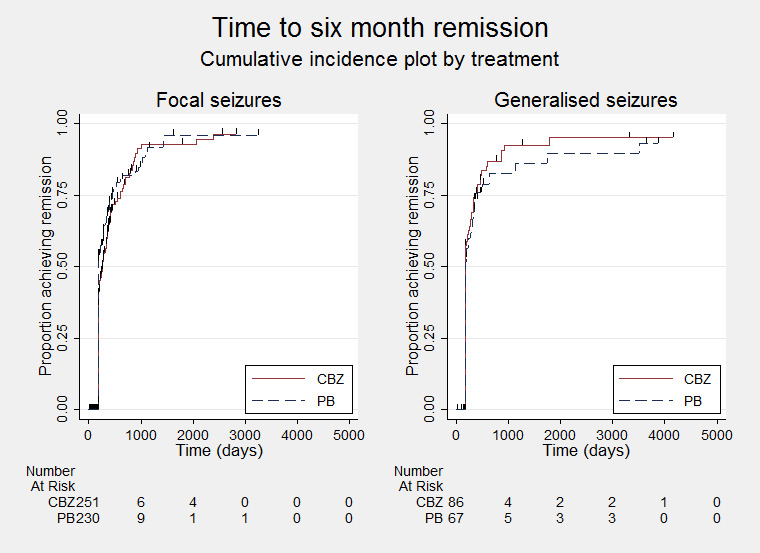
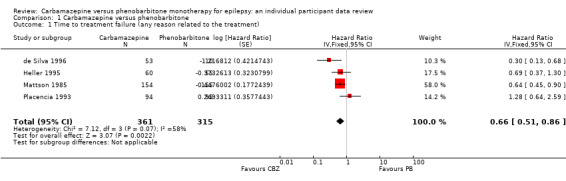
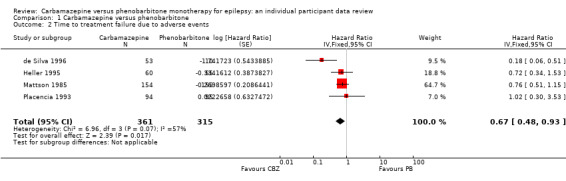
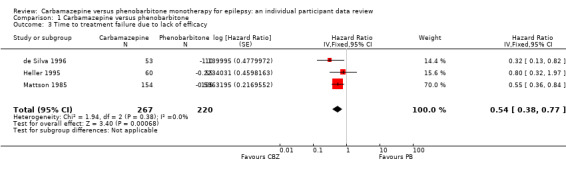
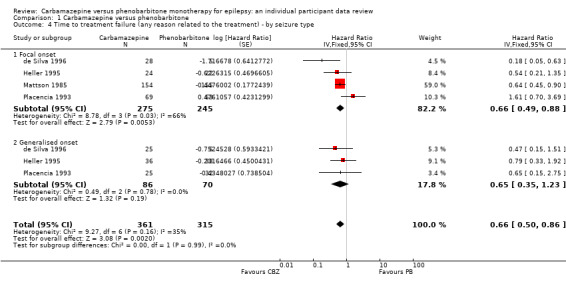
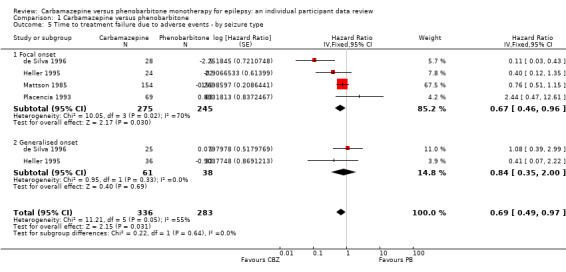
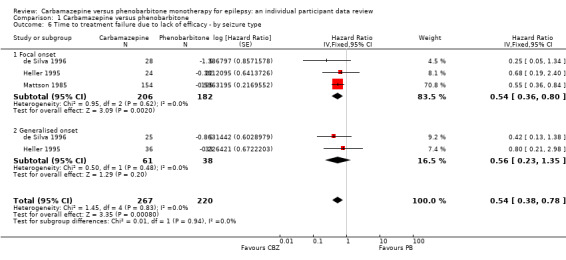
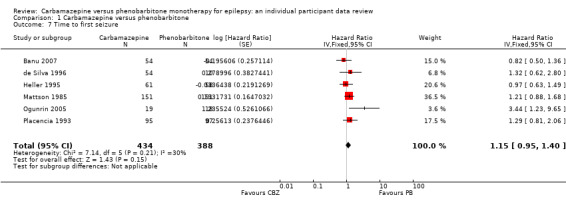
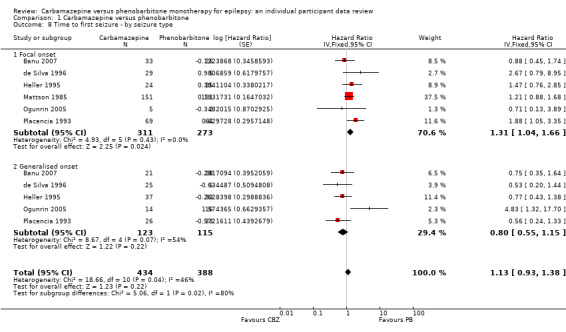
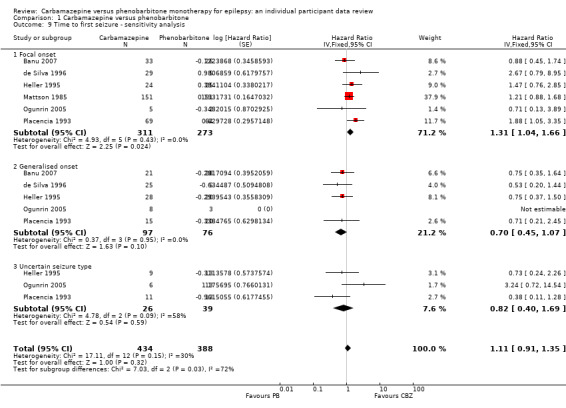
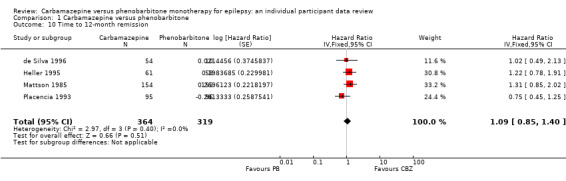
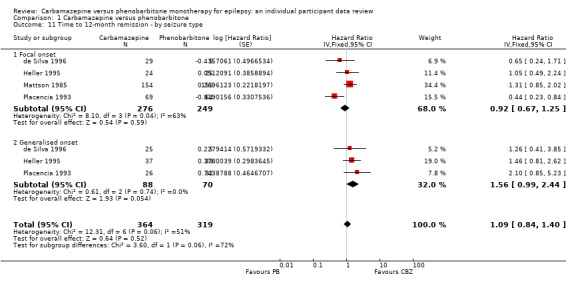
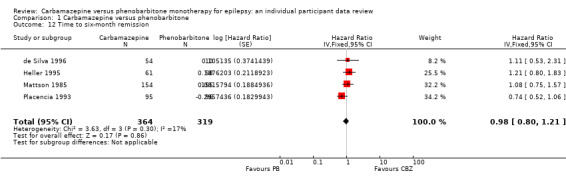
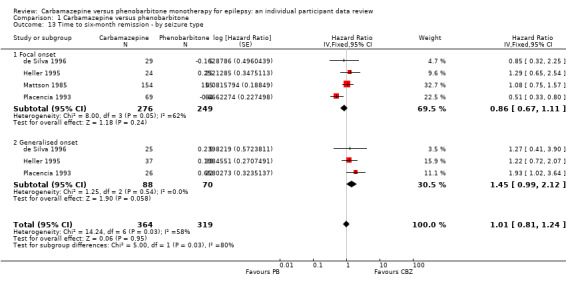
Main results: We included 13 trials in this review and IPD were available for 836 individuals out of 1455 eligible individuals from six trials, 57% of the potential data. For remission outcomes, a HR of less than 1 indicates an advantage for phenobarbitone and for first seizure and treatment failure outcomes a HR of less than 1 indicates an advantage for carbamazepine.Results for the primary outcome of the review were: time to treatment failure for any reason related to treatment (pooled HR adjusted for seizure type for 676 participants: 0.66, 95% CI 0.50 to 0.86, moderate-quality evidence), time to treatment failure due to adverse events (pooled HR adjusted for seizure type for 619 participants: 0.69, 95% CI 0.49 to 0.97, low-quality evidence), time to treatment failure due to lack of efficacy (pooled HR adjusted for seizure type for 487 participants: 0.54, 95% CI 0.38 to 0.78, moderate-quality evidence), showing a statistically significant advantage for carbamazepine compared to phenobarbitone.For our secondary outcomes, we did not find any statistically significant differences between carbamazepine and phenobarbitone: time to first seizure post-randomisation (pooled HR adjusted for seizure type for 822 participants: 1.13, 95% CI 0.93 to 1.38, moderate-quality evidence), time to 12-month remission (pooled HR adjusted for seizure type for 683 participants: 1.09, 95% CI 0.84 to 1.40, low-quality evidence), and time to six-month remission pooled HR adjusted for seizure type for 683 participants: 1.01, 95% CI 0.81 to 1.24, low-quality evidence).Results of these secondary outcomes suggest that there may be an association between treatment effect in terms of efficacy and seizure type; that is, that participants with focal onset seizures experience seizure recurrence later and hence remission of seizures earlier on phenobarbitone than carbamazepine, and vice versa for individuals with generalised seizures. It is likely that the analyses of these outcomes were confounded by several methodological issues and misclassification of seizure type, which could have introduced the heterogeneity and bias into the results of this review.Limited information was available regarding adverse events in the trials and we could not compare the rates of adverse events between carbamazepine and phenobarbitone. Some adverse events reported on both drugs were abdominal pain, nausea, and vomiting, drowsiness, motor and cognitive disturbances, dysmorphic side effects (such as rash), and behavioural side effects in three paediatric trials.
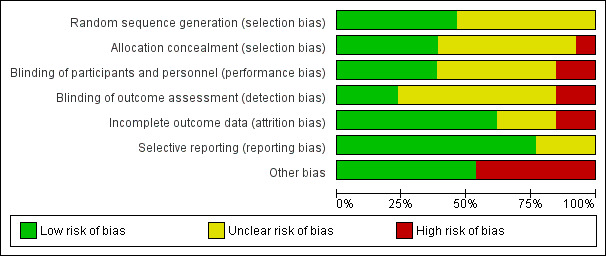
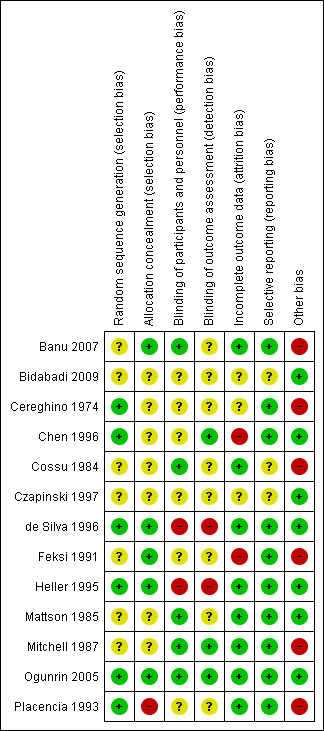
Authors' conclusions: Moderate-quality evidence from this review suggests that carbamazepine is likely to be a more effective drug than phenobarbitone in terms of treatment retention (treatment failures due to lack of efficacy or adverse events or both). Moderate- to low-quality evidence from this review also suggests an association between treatment efficacy and seizure type in terms of seizure recurrence and seizure remission, with an advantage for phenobarbitone for focal onset seizures and an advantage for carbamazepine for generalised onset seizures.However, some of the trials contributing to the analyses had methodological inadequacies and inconsistencies that may have impacted upon the results of this review. Therefore, we do not suggest that results of this review alone should form the basis of a treatment choice for a patient with newly onset seizures. We recommend that future trials should be designed to the highest quality possible with consideration of masking, choice of population, classification of seizure type, duration of follow-up, choice of outcomes and analysis, and presentation of results.
Conflict of interest statement
Sarah J Nevitt: nothing to declare
Anthony G Marson: a consortium of pharmaceutical companies (GSK, EISAI, UCB Pharma), funded the National Audit of Seizure Management in Hospitals (NASH), through grants paid to The University of Liverpool. Professor Tony Marson is part funded by National Institute for Health Research Collaboration for Leadership in Applied Health Research and Care North West Coast (NIHR CLAHRC NWC).
Catrin Tudur Smith: nothing to declare
Figures
Update of
-
Carbamazepine versus phenobarbitone monotherapy for epilepsy: an individual participant data review.Cochrane Database Syst Rev. 2016 Dec 15;12(12):CD001904. doi: 10.1002/14651858.CD001904.pub3. Cochrane Database Syst Rev. 2016. Update in: Cochrane Database Syst Rev. 2018 Oct 24;10:CD001904. doi: 10.1002/14651858.CD001904.pub4. PMID: 27976799 Free PMC article. Updated.
References
References to studies included in this review
Banu 2007 {published and unpublished data}
Bidabadi 2009 {unpublished data only}
-
- Bidabadi E. Comparison of the effects of phenobarbital versus carbamazepine as single drug therapy in partial seizure with secondary generalization in children. Epilepsia 2009;50 Suppl 10:167.
Cereghino 1974 {published data only}
Chen 1996 {published data only}
-
- Chen YJ, Kang WM, So WC. Comparison of antiepileptic drugs on cognitive function in newly diagnosed epileptic children: a psychometric and neurophysiological study. Epilepsia 1996;37(1):81‐6. - PubMed
Cossu 1984 {published data only}
-
- Cossu G, Monaco F, Piras MR, Grossi E. Short‐term therapy with carbamazepine and phenobarbital: effects on cognitive functioning in temporal lobe epilepsy [Trattamento a breve termine con carbamazepina e fenobarbital: effetto sulle funzioni mnesiche nell'epilessia temporale]. Bollettino Lega Italiana contro l'Epilessia 1984;45/46:377‐9.
Czapinski 1997 {unpublished data only}
-
- Czapinski P, Terczynski A, Czapinska E. Randomised 36‐month comparative study of valproic acid, phenytoin, phenobarbital and carbamazepine efficacy in patients with newly diagnosed epilepsy with partial complex seizures. Epilepsia 1997;38 Suppl(3):42.
de Silva 1996 {published and unpublished data}
-
- Silva M, MacArdle B, McGowan M, Hughes E, Stewart J, Neville BG, et al. Randomised comparative monotherapy trial of phenobarbitone, phenytoin, carbamazepine, or sodium valproate for newly diagnosed childhood epilepsy. Lancet 1996;347(9003):709‐13. - PubMed
Feksi 1991 {published and unpublished data}
-
- Feksi AT, Kaamugisha J, Sander JW, Gatiti S, Shorvon SD. Comprehensive primary health care antiepileptic drug treatment programme in rural and semi‐urban Kenya. ICBERG (International Community‐based Epilepsy Research Group). Lancet 1991;337(16):406‐9. - PubMed
Heller 1995 {published and unpublished data}
Mattson 1985 {published and unpublished data}
-
- Mattson RH, Cramer JA, Collins JF, Smith DB, Delgado‐Escueta AV, Browne TR, et al. Comparison of carbamazepine, phenobarbital, phenytoin, and primidone in partial and secondarily generalized tonic‐clonic seizures. New England Journal of Medicine 1985;313(3):145‐51. - PubMed
-
- Smith DB, Mattson RH, Cramer JA, Collins JF, Novelly RA, Craft B. Results of a nationwide Veterans Administration Cooperative Study comparing the efficacy and toxicity of carbamazepine, phenobarbital, phenytoin, and primidone. Epilepsia 1987;28(Suppl 3):50‐8. - PubMed
Mitchell 1987 {published data only}
-
- Mitchell WG, Chavez JM. Carbamazepine versus phenobarbital for partial onset seizures in children. Epilepsia 1987;28(1):56‐60. - PubMed
Ogunrin 2005 {published and unpublished data}
-
- Ogunrin O, Adamolekun B, Ogunniyi A. Cognitive effects of anti‐epileptic drugs in Nigerians with epilepsy. African Journal of Neurological Sciences 2005;24(1):18‐24.
Placencia 1993 {published and unpublished data}
-
- Placencia M, Sander JW, Shorvon SD, Roman M, Alarcon F, Bimos C, et al. Antiepileptic drug treatment in a community health care setting in northern Ecuador: a prospective 12‐month assessment. Epilepsy Research 1993;14(3):237‐44. - PubMed
References to studies excluded from this review
Bird 1966 {published data only}
-
- Bird CA, Griffin BP, Miklaszewska JM, Galbraith AW. Tegretol (carbamazepine): a controlled trial of a new anti‐convulsant. British Journal of Psychiatry 1966;112:737‐42.
Castro‐Gago 1998 {published data only}
-
- Castro‐Gago M, Eiris‐Punal J, Novo‐Rodriguez MI, Couceiro J, Camina F, Rodriguez‐Segade S. Serum carnitine levels in epileptic children before and during treatment with valproic acid, carbamazepine, and phenobarbital. Journal of Child Neurology 1998;13(11):546‐9. - PubMed
Hansen 1980 {published data only}
-
- Hansen BS, Dam M, Brandt J, Hvidberg EF, Angelo H, Christensen JM, et al. Influence of dextropropoxyphene on steady state serum levels and protein binding of three anti‐epileptic drugs in man. Acta Neurologica Scandinavica 1980;61(6):357‐67. - PubMed
Kuzuya 1993 {published data only}
-
- Kuzuya T, Hasegawa T, Shimizu K, Nabeshima T. Effect of anti‐epileptic drugs on serum zinc and copper concentrations in epileptic patients. International Journal of Clinical Pharmacology, Therapy, & Toxicology 1993;31(2):61‐5. - PubMed
Marjerrison 1968 {published data only}
-
- Marjerrison G, Jedlicki SM, Keogh RP, Hrychuk W, Poulakakis GM. Carbamazepine: behavioral, anticonvulsant and EEG effects in chronically‐hospitalized epileptics. Diseases of the Nervous System 1968;29(2):133‐6. - PubMed
Meador 1990 {published data only}
-
- Meador KJ, Loring DW, Huh K, Gallagher BB, King DW. Comparative cognitive effects of anticonvulsants. Neurology 1990;40:391‐4. - PubMed
Sabers 1995 {published data only}
-
- Sabers A, Moller A, Dam M, Smed A, Arlien‐Soborg P, Buchman J, et al. Cognitive function and anticonvulsant therapy: effect of monotherapy in epilepsy. Acta Neurologica Scandinavica 1995;92(1):19‐27. - PubMed
Additional references
Annegers 1999
-
- Annegers JF, Dubinsky S, Coan SP, Newmark ME, Roht L. The incidence of epilepsy and unprovoked seizures in multiethnic, urban health maintenance organizations. Epilepsia 1999;40(4):502‐6. - PubMed
Baulac 2002
-
- Baulac M, Cramer JA, Mattson RH. Phenobarbital and other barbiturates: adverse effects. In: Levy RH, Mattson RH, Meldrum BS, et al. editor(s). Antiepileptic Drugs. 5th Edition. Philadelphia: Lippincott Williams & Wilkins, 2002:528‐40.
Bromley 2014
Cockerell 1995
-
- Cockerell OC, Johnson AL, Sander JW, Hart YM, Shorvon SD. Remission of epilepsy: results from the National General Practice Study of Epilepsy. Lancet 1995;346(8968):140‐4. - PubMed
Commission 1981
-
- Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981;22(4):489‐501. - PubMed
Commission 1989
-
- Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 1989;30(4):389‐99. - PubMed
Gruber 1962
-
- Gruber CM, Brock JT, Dyken MD. Comparison of the effectiveness of phenobarbital, mephobarbital, primidone, dipheylhydantoin, ethotoin, metharbital, and methylphenylhydantion in motor seizures. Clinical Pharmacology and Therapeutics 1962;3:23‐8. - PubMed
Hauser 1993
-
- Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester, Minnesota 1935 ‐ 1984. Epilepsia 1993;34:453‐68. - PubMed
Higgins 2003
Higgins 2017
-
- Higgins JP, Altman DG, Sterne JA (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS (editors), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Hirtz 2007
-
- Hirtz D, Thurman DJ, Gwinn‐Hardy K, Mohamed M, Chaudhuri AR, Zalutsky R. How common are the "common" neurologic disorders?. Neurology 2007;68:326‐37. - PubMed
ILAE 1998
-
- ILAE Commission on Antiepileptic Drugs. Considerations on designing clinical trials to evaluate the place of new antiepileptic drugs in the treatment of newly diagnosed and chronic patients with epilepsy. Epilepsia 1998;39(7):799‐803. - PubMed
ILAE 2006
-
- Glauser T, Ben‐Menachem E, Bourgeois B, Cnaan A, Chadwick D, Guerreiro C, et al. ILAE treatment guidelines: evidence based analysis of antiepileptic drug efficacy and effectiveness as initial monotherapy for epileptic seizures and syndromes. Epilepsia 2006;47(7):1094‐120. - PubMed
Jones 1996
Juul‐Jenson 1983
-
- Juul‐Jenson P, Foldspang A. Natural history of epileptic seizures. Epilepsia 1983;24:297‐312. - PubMed
Kirkham 2010
-
- Kirkham JJ, Dwan KM, Altman DG, Gamble C, Dodd S, Smyth R, et al. The impact of outcome reporting bias in randomised controlled trials on a cohort of systematic reviews. BMJ 2010;340:c365. - PubMed
Kwan 2000
-
- Kwan P, Brodie MJ. Early identification of refractory epilepsy. New England Journal of Medicine 2000;342:314‐9. - PubMed
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Liporace 1994
-
- Liporace JD, Sperling MR, Dichter MA. Absence seizures and carbamazepine in adults. Epilepsia 1994;35(5):1026‐8. - PubMed
MacDonald 1995
-
- MacDonald RL, Kelly KM. Antiepileptic drug mechanisms of action. Epilepsia 1995;36(Suppl 2):S2‐12. - PubMed
MacDonald 2000
-
- MacDonald BK, Johnson AL, Goodridge DM, Cockerell OC, Sander JWA, Shorvon SD. Factors predicting prognosis of epilepsy after presentation with seizures. Annals of Neurology 2000;48:833‐41. - PubMed
Malafosse 1994
-
- Malfosse A, Genton P, Hirsch E, Marescaux C, Broglin D, Bernasconi R. Idiopathic Generalised Epilepsies: Clinical, Experimental and Genetic. Eastleigh: John Libbey and Company, 1994.
Marson 2000
Matlow 2012
Meador 2008
Moher 2009
Morrow 2006
Murray 1994
-
- Murray CJL, Lopez AD. Global comparative assessments in the health sector. World Health Organization. Geneva, 1994.
Nevitt 2017a
Nevitt 2017b
Nevitt 2018a
Nevitt 2018b
Nevitt 2018c
Ngugi 2010
NICE 2012
-
- National Institute for Health and Care Excellence. The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care; Clinical Guidance 137. London: National Institute for Health and Care Excellence, 2012.
Nolan 2013a
-
- Nolan SJ, Sutton L, Marson A, Tudur Smith C. Consistency of outcome and statistical reporting of time‐to‐event data: the impact on Cochrane Reviews and meta‐analyses in epilepsy. 21st Cochrane Colloquium: Better Knowledge for Better Health. Quebec City, 2013:114‐5.
Nolan 2013c
Nolan 2016b
Olafsson 2005
-
- Olafsson E, Ludvigsson P, Gudmundsson G, Hesdorfer D, Kjartansson O, Hauser WA. Incidence of unprovoked seizures and epilepsy in Iceland and assessment of the epilepsy syndrome classification: a prospective study. Lancet Neurology 2005;4:627‐34. - PubMed
Pal 1998
-
- Pal DK, Das T, Chaudhury G, Johnson AL, Neville BG. Randomised controlled trial to assess acceptability of phenobarbital for childhood epilepsy in rural India. Lancet 1998;351(9095):19‐23. - PubMed
Parmar 1998
-
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta‐analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815‐34. - PubMed
Ragsdale 1991
-
- Ragsdale DS, Scheuer T, Catterall WA. Frequency and voltage dependent inhibition of type hA Naı channels, expressed in a mammalian cell line, by local anesthetic, antiarrhythmic, and anticonvulsant drugs. Molecular Pharmacology 1991;40:756‐65. - PubMed
Rho 1996
Sander 1996
Sander 2004
-
- Sander JW. The use of anti‐epileptic drugs ‐ principles and practice. Epilepsia 2004;45(6):28‐34. - PubMed
Scheffer 2017
Shakir 1980
-
- Shakir RA. Sodium valproate, phenytoin and carbamazepine as sole anticonvulsants. The place of sodium valproate in the treatment of epilepsy. London: Academic Press Inc (London) Ltd and the Royal Society of Medicine, 1980:7‐16.
Shields 1983
-
- Shields WD, Saslow E. Myoclonic, atonic, and absence seizures following institution of carbamazepine therapy in children. Neurology 1983;33:1487‐9. - PubMed
Snead 1985
-
- Snead OC, Hosey LC. Exacerbation of seizures in children by carbamazepine. New England Journal of Medicine 1985;313:916‐21. - PubMed
Stata 2015 [Computer program]
-
- StataCorp LP. Stata Statistical Software. Version release 14. CollegeStation, TX: StataCorp LP, 2015.
Trimble 1988
-
- Trimble MR, Cull C. Children of school age: the influence of antiepileptic drugs on behavior and intellect. Epilepsia 1988;29(Suppl 3):S15‐19. - PubMed
Tudur Smith 2007
Wallace 1997
-
- Wallace H, Shorvon SD, Hopkins A, O'Donoghue M. Guidelines for the Clinical Management of Adults with Poorly Controlled Epilepsy. London: Royal College of Physicians, 1997.
Weston 2016
Williamson 2000
-
- Williamson PR, Marson AG, Tudur C, Hutton JL, Chadwick DW. Individual patient data meta‐analysis of randomized anti‐epileptic drug monotherapy trials. Journal of Evaluation in Clinical Practice 2000;6(2):205‐14. - PubMed
Williamson 2002
-
- Williamson PR, Tudur Smith C, Hutton JL, Marson AG. Aggregate data meta‐analysis with time‐to‐event outcomes. Statistics in Medicine 2002;21(11):3337‐51. - PubMed
References to other published versions of this review
Nolan 2015
Nolan 2016a
Tudur 2000
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources