

Acute Exacerbation of Chronic Obstructive Pulmonary Disease and Subsequent Risk of Emergency Department Visits and Hospitalizations for Atrial Fibrillation
- PMID: 30354294
- PMCID: PMC7735661
- DOI: 10.1161/CIRCEP.118.006322
Acute Exacerbation of Chronic Obstructive Pulmonary Disease and Subsequent Risk of Emergency Department Visits and Hospitalizations for Atrial Fibrillation
Erratum in
-
Correction to: Acute Exacerbation of Chronic Obstructive Pulmonary Disease and Subsequent Risk of Emergency Department Visits and Hospitalizations for Atrial Fibrillation.Circ Arrhythm Electrophysiol. 2018 Oct;11(10):e000033. doi: 10.1161/HAE.0000000000000033. Circ Arrhythm Electrophysiol. 2018. PMID: 30354412 No abstract available.
Abstract
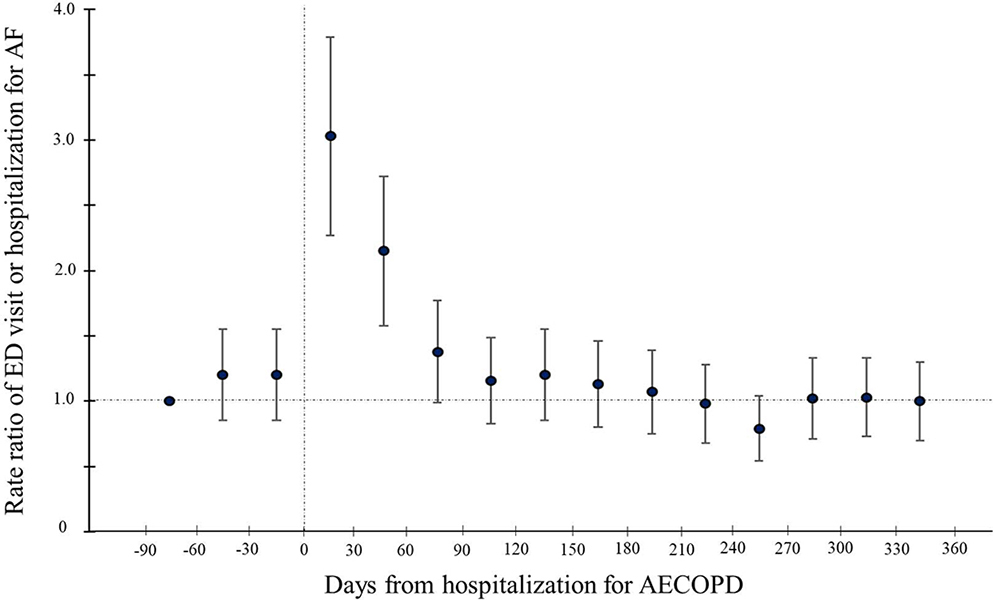
Background Although emerging evidence has suggested the relationship of chronic obstructive pulmonary disease with atrial fibrillation (AF), little is known about whether acute exacerbation of chronic obstructive pulmonary disease (AECOPD) increases the risk of repeated AF-related healthcare utilization. Methods This is a self-controlled case series study using the population-based emergency department (ED) and inpatient databases of 5 US states from 2007 through 2012. Among patients with existing AF, we identified patients with an AECOPD hospitalization and at least 1 ED visit or hospitalization for AF during the observation period. We constructed conditional Poisson regression models to compare the rate of AF-related ED visits or hospitalizations during sequential 90-day periods after the AECOPD hospitalization, with pre-AECOPD days 1 to 90 as the reference. Results We analyzed 944 patients who were hospitalized for AECOPD and had an ED visit or hospitalization for AF during a 450-day period. The median age was 77 years, and 41% were men. Compared with the reference period, the rate of AF-related ED visits or hospitalizations significantly increased in the post-AECOPD days 1 to 90 (7.3 versus 14.1 per 100 person-months; rate ratio, 1.93; 95% CI, 1.63-2.29; P<0.001). Then, the rate decreased to the reference level in the post-AECOPD days 91 to 180 (7.5 per 100 person-months; rate ratio, 1.03; 95% CI, 0.85-1.25; P=0.77) and remained at the reference level during post-AECOPD days 181 to 270 (rate ratio, 0.84; 95% CI, 0.68-1.03; P=0.09) and days 271 to 360 (rate ratio, 0.90; 95% CI, 0.73-1.10; P=0.29). These temporal associations persisted with stratification by age, sex, and season. Conclusions Among patients with existing AF, AECOPD was associated with a higher risk of AF-related ED visit or hospitalization in the first 90-day post-AECOPD period.
Keywords: aged; atrial fibrillation; epidemiology; humans; pulmonary disease, chronic obstructive.
Figures

References
-
- Agency for Healthcare Research and Quality. HCUP net. http://hcupnet.ahrq.gov/. Accessed May 1, 2018
-
- Steinberg BA, Kim S, Fonarow GC, Thomas L, Ansell J, Kowey PR, Mahaffey KW, Gersh BJ, Hylek E, Naccarelli G, Go AS, Reiffel J, Chang P, Peterson ED and Piccini JP. Drivers of hospitalization for patients with atrial fibrillation: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF). Am Heart J 2014;167:735–42.e2. - PMC - PubMed
-
- Patel NJ, Deshmukh A, Pant S, Singh V, Patel N, Arora S, Shah N, Chothani A, Savani GT, Mehta K, Parikh V, Rathod A, Badheka AO, Lafferty J, Kowalski M, Mehta JL, Mitrani RD, Viles-Gonzalez JF and Paydak H. Contemporary trends of hospitalization for atrial fibrillation in the United States, 2000 through 2010: implications for healthcare planning. Circulation. 2014;129:2371–9. - PubMed
-
- Buch P, Friberg J, Scharling H, Lange P and Prescott E. Reduced lung function and risk of atrial fibrillation in the Copenhagen City Heart Study. Eur Respir J. 2003;21:1012–1016. - PubMed
-
- Shibata Y, Watanabe T, Osaka D, Abe S, Inoue S, Tokairin Y, Igarashi A, Yamauchi K, Kimura T, Kishi H, Aida Y, Nunomiya K, Nemoto T, Sato M, Konta T, Kawata S, Kato T, Kayama T and Kubota I. Impairment of pulmonary function is an independent risk factor for atrial fibrillation: the Takahata study. Int J Med Sci 2011;8:514–22. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
