

Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015
- PMID: 30354376
- PMCID: PMC6428412
- DOI: 10.1161/CIRCOUTCOMES.118.004689
Population-Based Assessment of the Incidence of Aortic Dissection, Intramural Hematoma, and Penetrating Ulcer, and Its Associated Mortality From 1995 to 2015
Abstract
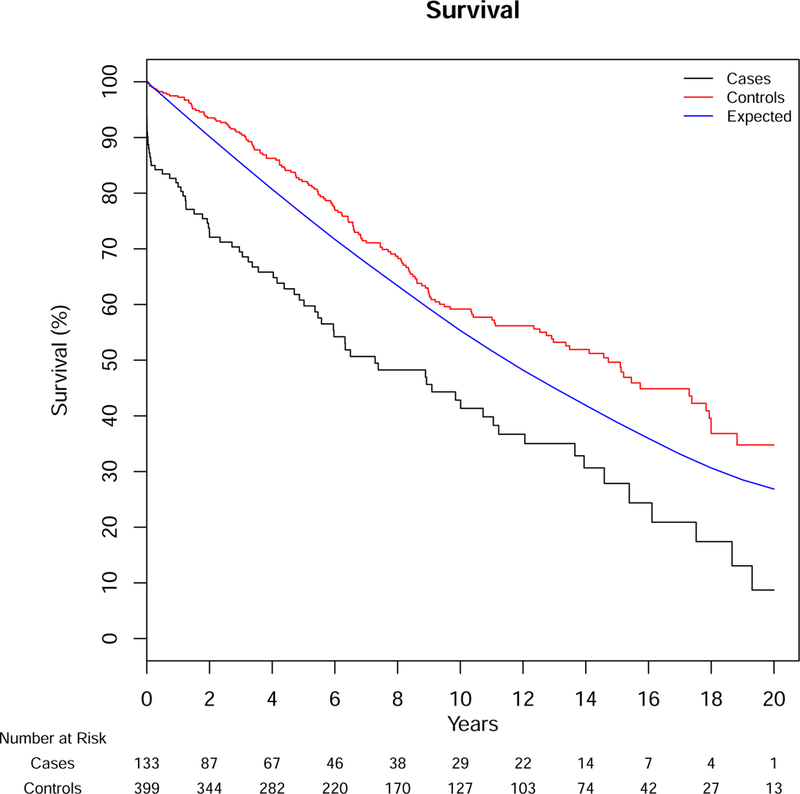
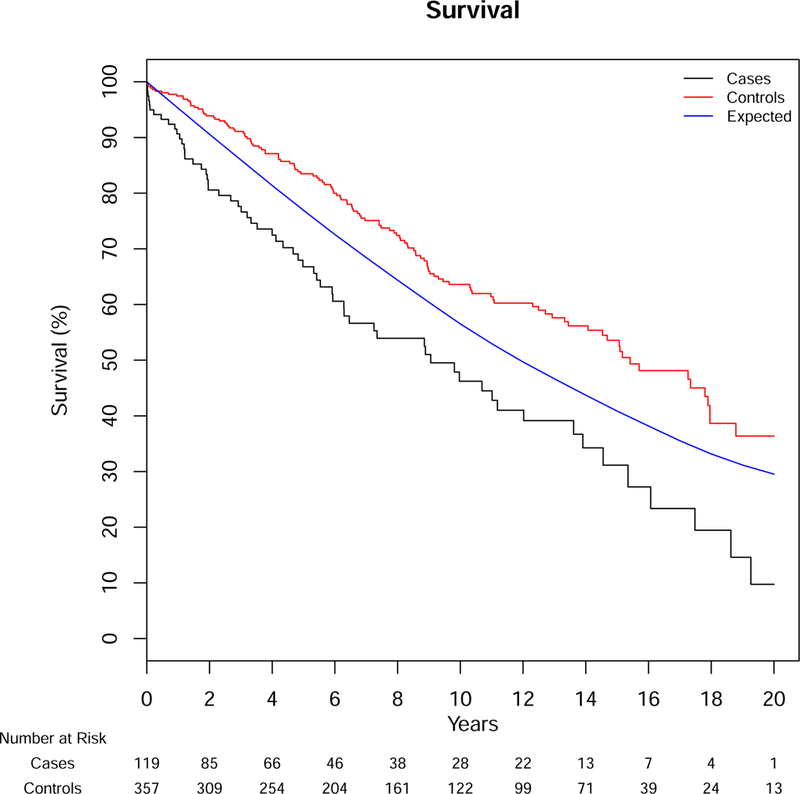
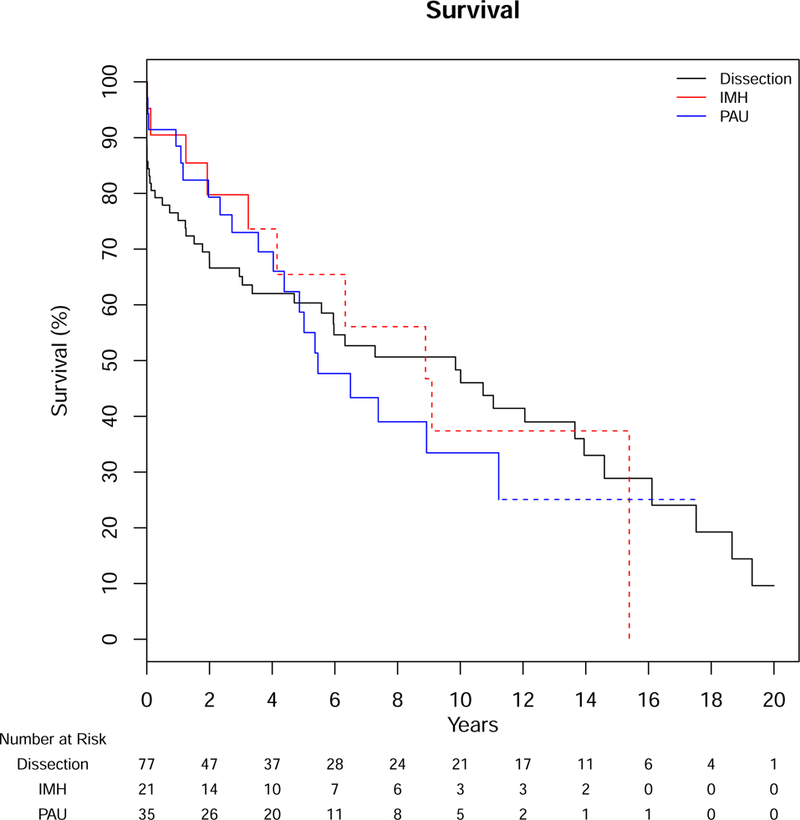
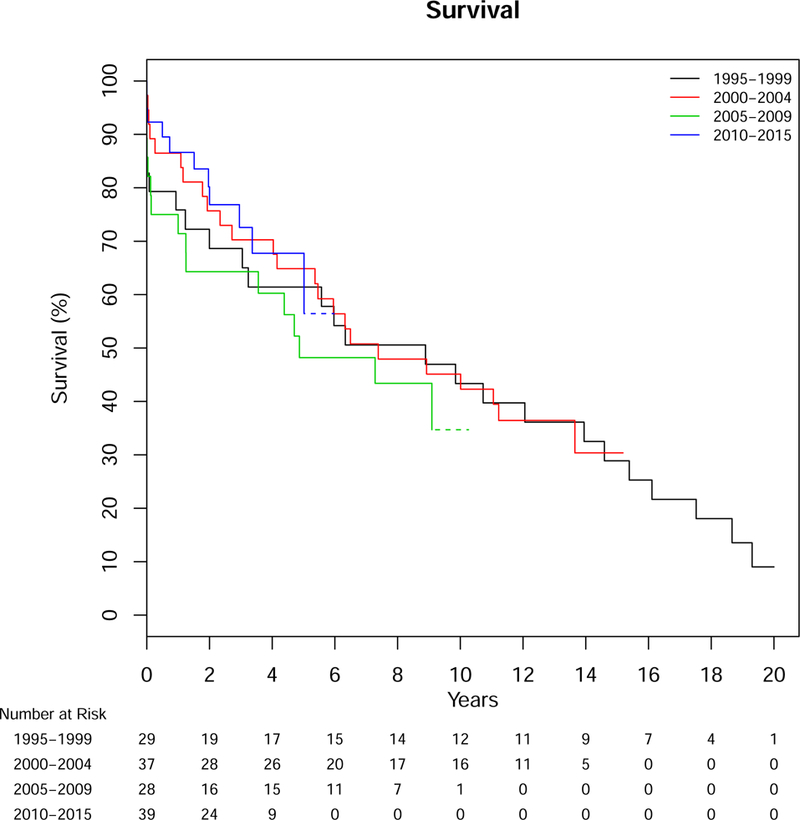
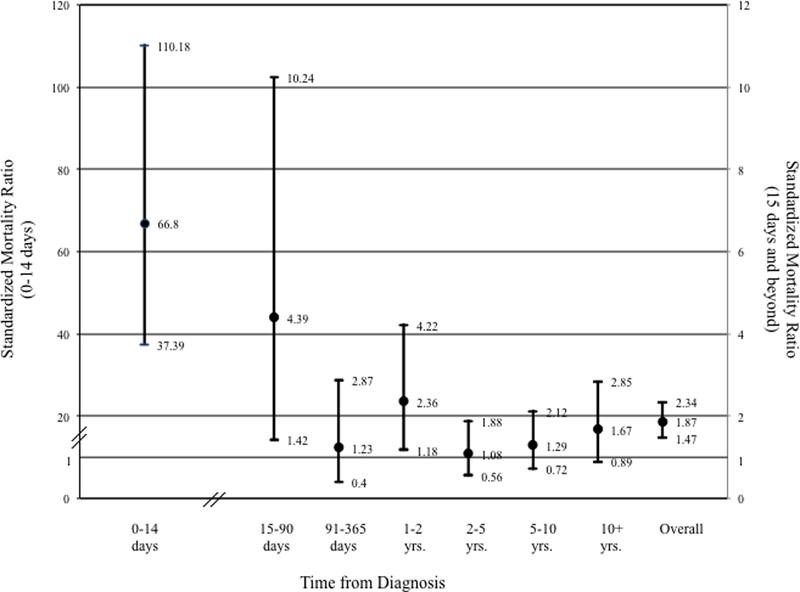
Background Aortic syndromes (ASs), including aortic dissection, intramural hematoma, and penetrating aortic ulcer, carry significant acute and long-term morbidity and mortality. However, the contemporary incidence and outcomes of AS are unknown. Methods and Results We used the Rochester Epidemiology Project record linkage system to identify all Olmsted County, MN, residents with AS (1995-2015). Diagnostic imaging, medical records, and death certificates were reviewed to confirm the diagnosis and AS subtype. Age- and sex-adjusted incidence rates were estimated using annual county-level census data. Survival for patients with AS was compared with age- and sex-matched controls using Cox regression to adjust for comorbid conditions. We identified 133 patients with AS (77, aortic dissection; 21, intramural hematoma; and 35, penetrating aortic ulcer). Average age was 71.8 years (SD=14.1), and 57% were men. The age- and sex-adjusted incidence was 7.7 per 100 000 person-years, was higher for men than women (10.2 versus 5.7 per 100 000 person-years), and increased with age. Among subtypes, the incidence of aortic dissection was highest (4.4 per 100 000 person-years), whereas the incidence of penetrating aortic ulcer and intramural hematoma was lower (2.1 and 1.2 per 100 000 person-years). Overall, the incidence of AS was stable over time ( P trend=0.33), although the incidence of penetrating aortic ulcer seemed to increase from 0.6 to 2.6 per 100 000 person-years ( P=0.008) with variability over the study interval. Patients with AS had more than twice the mortality rate at 5, 10, and 20 years when compared with population-based controls (5-, 10-, and 20-year mortality 39%, 57%, and 91% versus 18%, 41%, and 66%; overall adjusted mortality hazards ratio=2.1; P<0.001). Survival was lower than expected up to 90 days after AS diagnosis and did not differ significantly by subtype or by 5-year strata of diagnosis. Conclusions Overall, the incidence of aortic dissection and intramural hematoma has remained stable since 1995, despite the decline noted for other cardiovascular disease. AS confers increased early and long-term mortality that has not changed. These data highlight the need to improve long-term care to impact the prognosis of this patient group.
Keywords: dissection; epidemiology; hematoma; incidence; syndrome.
Figures
References
-
- Hirst AE Jr., Johns Jr. and Kime SW Jr. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine 1958;37:217–79. - PubMed
-
- Nienaber CA and Eagle KA. Aortic dissection: new frontiers in diagnosis and management: Part I: from etiology to diagnostic strategies. Circulation 2003;108:628–35. - PubMed
-
- Clouse WD, Hallett JW Jr., Schaff HV, Spittell PC, Rowland CM, Ilstrup DM and Melton LJ 3rd. Acute aortic dissection: population-based incidence compared with degenerative aortic aneurysm rupture. Mayo Clinic proceedings 2004;79:176–80. - PubMed
-
- Hagan PG, Nienaber CA, Isselbacher EM, Bruckman D, Karavite DJ, Russman PL, Evangelista A, Fattori R, Suzuki T, Oh JK, Moore AG, Malouf JF, Pape LA, Gaca C, Sechtem U, Lenferink S, Deutsch HJ, Diedrichs H, Marcos y Robles J, Llovet A, Gilon D, Das SK, Armstrong WF, Deeb GM and Eagle KA. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA : the journal of the American Medical Association 2000;283:897–903. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
