

Coronary Computed Tomography Angiography-Specific Definitions of High-Risk Plaque Features Improve Detection of Acute Coronary Syndrome
- PMID: 30354493
- PMCID: PMC6205220
- DOI: 10.1161/CIRCIMAGING.118.007657
Coronary Computed Tomography Angiography-Specific Definitions of High-Risk Plaque Features Improve Detection of Acute Coronary Syndrome
Abstract
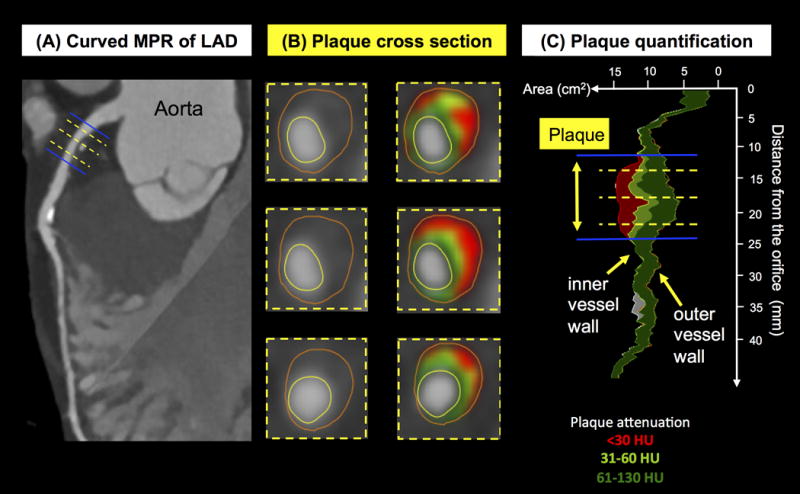
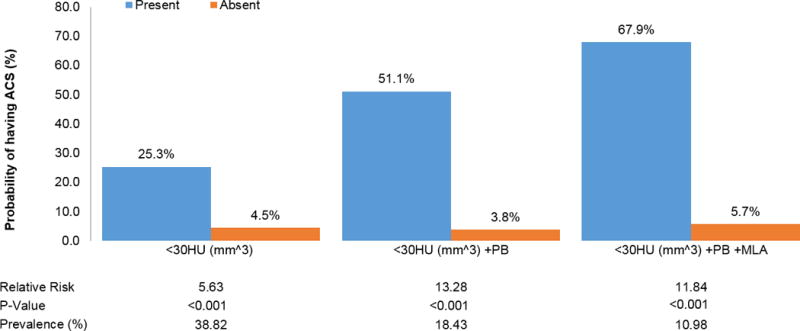
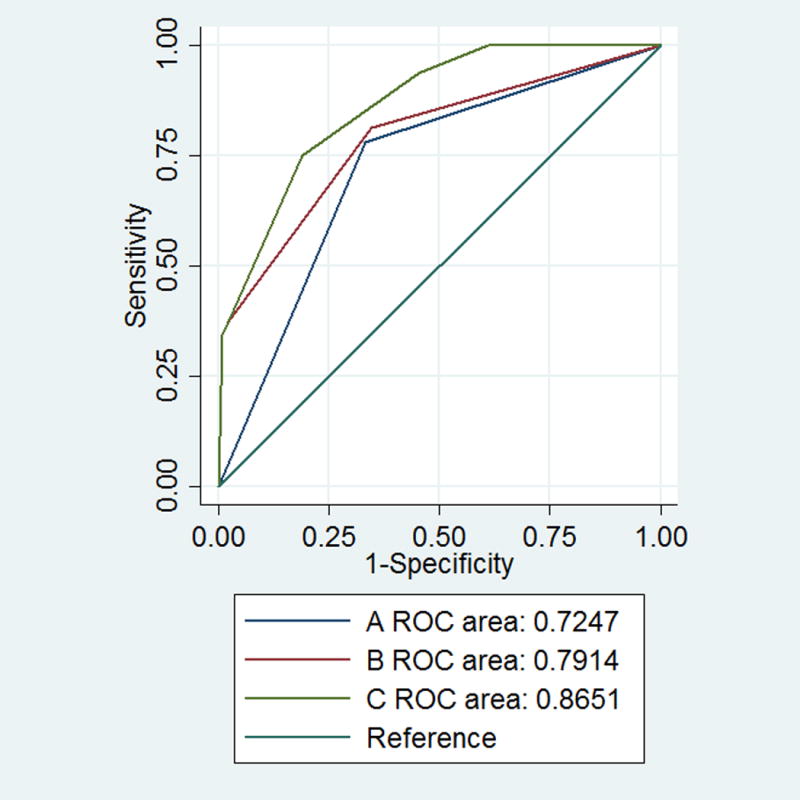
Background High-risk plaque (HRP) features as detected by coronary computed tomography angiography (CTA) predict acute coronary syndrome (ACS). We sought to determine whether coronary CTA-specific definitions of HRP improve discrimination of patients with ACS as compared with definitions from intravascular ultrasound (IVUS). Methods and Results In patients with suspected ACS, randomized to coronary CTA in the ROMICAT II (Rule Out Myocardial Infarction/Ischemia Using Computer Assisted Tomography II) trial, we retrospectively performed semiautomated quantitative analysis of HRP (including remodeling index, plaque burden as derived by plaque area, low computed tomography attenuation plaque volume) and degree of luminal stenosis and analyzed the performance of traditional IVUS thresholds to detect ACS. Furthermore, we derived CTA-specific thresholds in patients with ACS to detect culprit lesions and applied those to all patients to calculate the discriminatory ability to detect ACS in comparison to IVUS thresholds. Of 472 patients, 255 patients (56±7.8 years; 63% men) had coronary plaque. In 32 patients (6.8%) with ACS, culprit plaques (n=35) differed from nonculprit plaques (n=172) with significantly greater values for all HRP features except minimal luminal area (significantly lower; all P<0.01). IVUS definitions showed good performance while minimal luminal area (odds ratio: 6.82; P=0.014) and plaque burden (odds ratio: 5.71; P=0.008) were independently associated with ACS but not remodeling index (odds ratio: 0.78; P=0.673). Optimized CTA-specific thresholds for plaque burden (area under the curve: 0.832 versus 0.676) and degree of stenosis (area under the curve: 0.826 versus 0.721) showed significantly higher diagnostic performance for ACS as compared with IVUS-based thresholds (all P<0.05) with borderline significance for minimal luminal area (area under the curve: 0.817 versus 0.742; P=0.066). Conclusions CTA-specific definitions of HRP features may improve the discrimination of patients with ACS as compared with IVUS-based definitions. CLINICAL TRIAL REGISTRATION URL: https://www.clinicaltrials.gov . Unique identifier: NCT01084239.
Keywords: acute coronary syndrome; angiography; computed tomography angiography; coronary angiography; myocardial ischemia; tomography, X-ray computed; ultrasonography, intravascular.
Figures

Comment in
-
Plaque Assessment Using Computed Tomography Angiography.Circ Cardiovasc Imaging. 2018 Aug;11(8):e008146. doi: 10.1161/CIRCIMAGING.118.008146. Circ Cardiovasc Imaging. 2018. PMID: 30354503 No abstract available.
References
-
- Motoyama S, Sarai M, Harigaya H, Anno H, Inoue K, Hara T, Naruse H, Ishii J, Hishida H, Wong ND, Virmani R, Kondo T, Ozaki Y, Narula J. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol. 2009;54:49–57. - PubMed
-
- Hoffmann U, Moselewski F, Nieman K, Jang IK, Ferencik M, Rahman AM, Cury RC, Abbara S, Joneidi-Jafari H, Achenbach S, Brady TJ. Noninvasive assessment of plaque morphology and composition in culprit and stable lesions in acute coronary syndrome and stable lesions in stable angina by multidetector computed tomography. J Am Coll Cardiol. 2006;47:1655–62. - PubMed
-
- Puchner SB, Liu T, Mayrhofer T, Truong QA, Lee H, Fleg JL, Nagurney JT, Udelson JE, Hoffmann U, Ferencik M. High-risk plaque detected on coronary CT angiography predicts acute coronary syndromes independent of significant stenosis in acute chest pain: results from the ROMICAT-II trial. J Am Coll Cardiol. 2014;64:684–92. - PMC - PubMed
-
- Pflederer T, Marwan M, Schepis T, Ropers D, Seltmann M, Muschiol G, Daniel WG, Achenbach S. Characterization of culprit lesions in acute coronary syndromes using coronary dual-source CT angiography. Atherosclerosis. 2010;211:437–44. - PubMed
-
- Maurovich-Horvat P, Ferencik M, Voros S, Merkely B, Hoffmann U. Comprehensive plaque assessment by coronary CT angiography. Nat Rev Cardiol. 2014;11:390–402. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
