

Point-of-care CRP matters: normal CRP levels reduce immediate antibiotic prescribing for acutely ill children in primary care: a cluster randomized controlled trial
- PMID: 30354904
- PMCID: PMC6381547
- DOI: 10.1080/02813432.2018.1529900
Point-of-care CRP matters: normal CRP levels reduce immediate antibiotic prescribing for acutely ill children in primary care: a cluster randomized controlled trial
Abstract
Objective: Antibiotics are prescribed too often in acutely ill children in primary care. We examined whether a Point-of-Care (POC) C-reactive Protein (CRP) test influences the family physicians' (FP) prescribing rate and adherence to the Evidence Based Medicine (EBM) practice guidelines.
Design: Cluster randomized controlled trial.
Setting: Primary care, Flanders, Belgium.
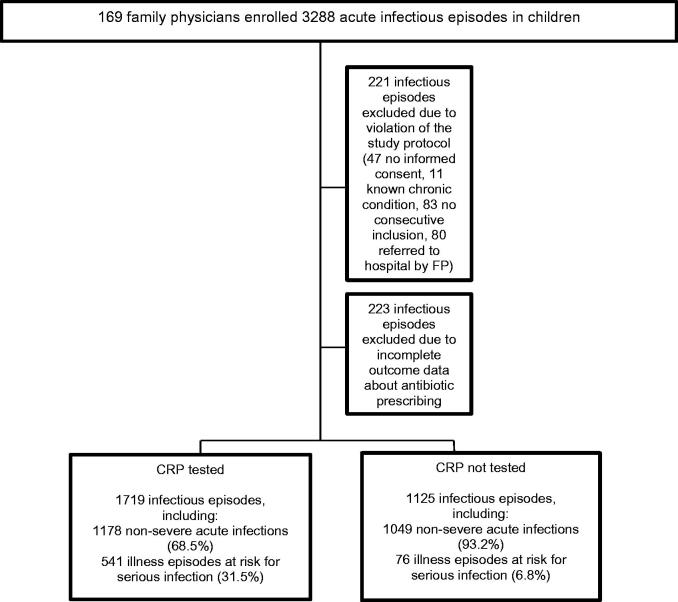
Intervention: Half of the children with non-severe acute infections (random allocation of practices to perform POC CRP or not) and all children at risk for serious infection were tested with POC CRP.
Subjects: Acutely ill children consulting their FP.
Main outcome measure: Immediate antibiotic prescribing.
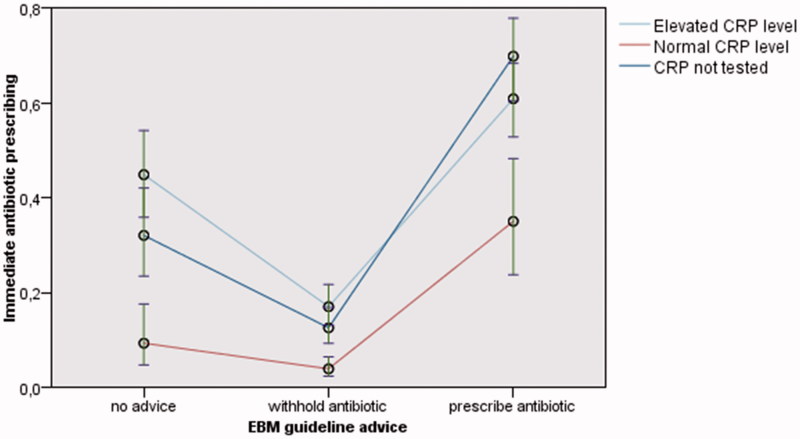
Results: 2844 infectious episodes recruited by 133 FPs between 15 February 2013 and 28 February 2014 were analyzed. A mixed logistic regression analysis was performed. Compared to episodes in which CRP was not tested, the mere performing of POC CRP reduced prescribing in case EBM practice guidelines advise to prescribe antibiotics (adjusted odds ratio (aOR) 0.54 (95% Confidence Interval (CI) 0.33-0.90). Normal CRP levels reduced antibiotic prescribing, regardless of whether the advice was to prescribe (aOR 0.24 (95%CI 0.11-0.50) or to withhold (aOR 0.31 (95%CI 0.17-0.57)). Elevated CRP levels did not increase antibiotic prescribing.
Conclusion: Normal CRP levels discourage immediate antibiotic prescribing, even when EBM practice guidelines advise differently. Most likely, a normal CRP convinces FPs to withhold antibiotics when guidelines go against their own gut feeling. Future research should focus on whether POC CRP can effectively identify children that benefit from antibiotics more accurately, without increasing the risks of under-prescribing. Key points What is previously known or believed on this topic •Antibiotics are prescribed too often for non-severe conditions. Point-of-care (POC) C-reactive Protein (CRP) testing without guidance does not reduce immediate antibiotic prescribing in acutely ill children in primary care. What this research adds •FPs clearly consider CRP once available: normal CRP levels discourage immediate antibiotic prescribing, even when EBM practice guidelines advise differently. Most likely, a normal CRP convinces FPs to withhold antibiotics when guidelines go against their own gut feeling. •Future research should focus on whether POC CRP can effectively identify children that benefit from antibiotics more accurately, without increasing the risks of under-prescribing.
Keywords: Anti-Bacterial Agents/therapeutic use; C-reactive protein/analysis; Randomized controlled trial; acute disease; child; point-of-care-systems.
Figures

References
-
- M Van de Casteele. Numbers of reimbursement of antibiotics for children in outpatient care. In: National Institute for Health and Disability Insurance (RIZIV). Consensus meeting June 2th 2016. The rational use of antibiotics for the child in outpatient care. [In Dutch]. Brussels: RIZIV, 2016: 42–53. http://www.riziv.fgov.be/SiteCollectionDocuments/consensus_sprekersbroch... (accessed 23 Jan 2018).
-
- Cabral C, Lucas PJ, Ingram J, Hay AD, et al. “It's safer to …” parent consulting and clinician antibiotic prescribing decisions for children with respiratory tract infections: an analysis across four qualitative studies. Soc Sci Med. 2015;136-137:156–164. - PubMed
-
- Mainous AG 3rd, Hueston WJ, Love MM. Antibiotics for colds in children: who are the high prescribers? Arch Pediatr Adolesc Med. 1998;152(4):349–352. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous