

Review
doi: 10.1056/NEJMra1413485.
Aplastic Anemia
Affiliations
- PMID: 30354958
- PMCID: PMC6467577
- DOI: 10.1056/NEJMra1413485
Item in Clipboard
Review
Aplastic Anemia
N Engl J Med.
.
No abstract available
Figures
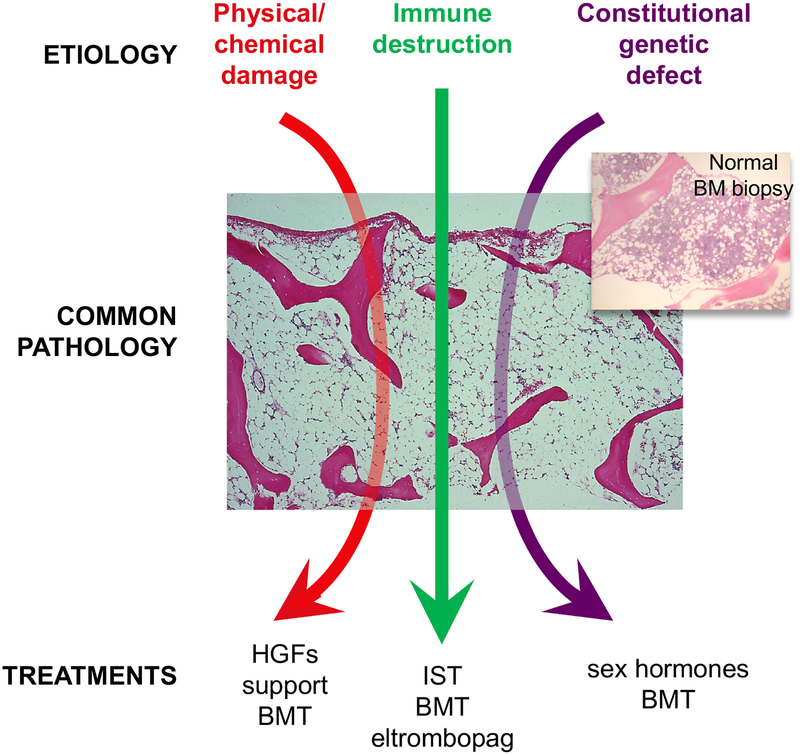
Pathophysiologies of aplastic anemia. The common pathology of the bone marrow replaced by fat can result from chemical or physical damage (iatrogenic; benzene); immune destruction (mainly T cells); and as a constitutional defect in genes important in maintenance of cell integrity and immune regulation. HGF=hematopoietic growth factors; BMT= bone marrow transplantation; IST=immunosuppression.
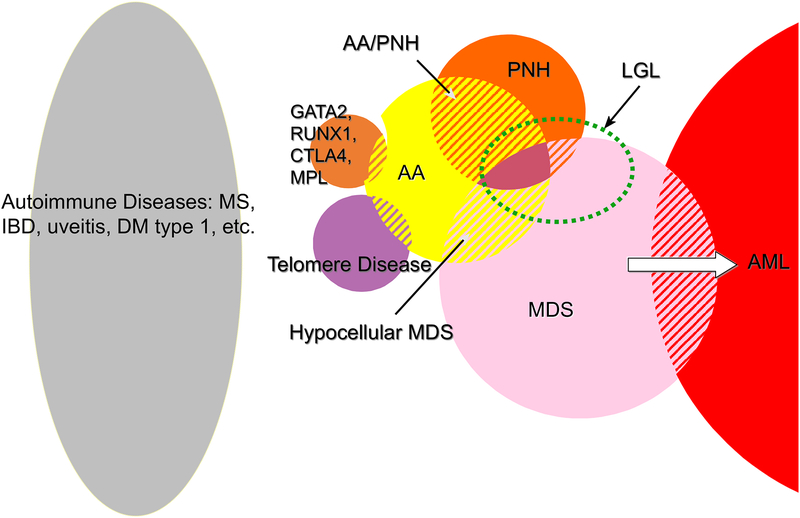
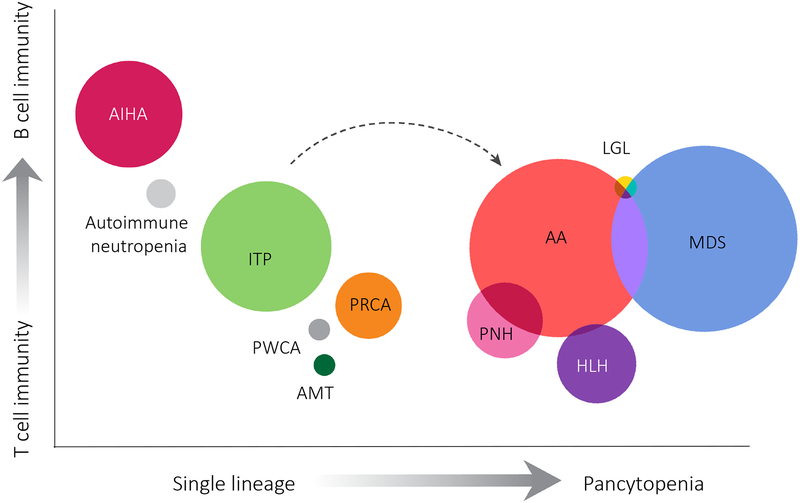
Aplastic anemia in relationship to other diseases. A) Venn diagram emphasizing overlap of aplastic anemia, both diagnostic and pathophysiologic, with PNH, MDS, and constitutional marrow failure syndromes, as well as to other immune-mediated diseases in which a single organ is targeted. B) Spectrum of immune cytopenias. The consensus for dominant immune effectors is delineated on the y axis; for examples, autoimmune peripheral blood cell destruction is mainly antibody mediated, whereas T cells have been implicated in marrow destruction. However, the immune response is almost certainly complex in all these diseases. AA=aplastic anemia; PNH=paroxysmal nocturnal hemoglobinuria; LGL=large granular lymphocytosis; MDS=myelodysplastic syndromes; AML=acute myeloid leukemia; MS=multiple sclerosis; IBD=inflammatory bowel disease; DM=diabetes mellitus; ITP= immune thrombocytopenic purpura; AIHA=autoimmune hemolytic anemia; PRCA=pure red cell aplasia; PWCA=pure white cell aplasia; AMT=amegakaryocytic thrombocytopenia; HLH=hemophagocytic lymphohistiocytosis. (For schematic purposes the circles in the Venn diagram have been scaled to PubMed citations.)
Aplastic anemia in relationship to other diseases. A) Venn diagram emphasizing overlap of aplastic anemia, both diagnostic and pathophysiologic, with PNH, MDS, and constitutional marrow failure syndromes, as well as to other immune-mediated diseases in which a single organ is targeted. B) Spectrum of immune cytopenias. The consensus for dominant immune effectors is delineated on the y axis; for examples, autoimmune peripheral blood cell destruction is mainly antibody mediated, whereas T cells have been implicated in marrow destruction. However, the immune response is almost certainly complex in all these diseases. AA=aplastic anemia; PNH=paroxysmal nocturnal hemoglobinuria; LGL=large granular lymphocytosis; MDS=myelodysplastic syndromes; AML=acute myeloid leukemia; MS=multiple sclerosis; IBD=inflammatory bowel disease; DM=diabetes mellitus; ITP= immune thrombocytopenic purpura; AIHA=autoimmune hemolytic anemia; PRCA=pure red cell aplasia; PWCA=pure white cell aplasia; AMT=amegakaryocytic thrombocytopenia; HLH=hemophagocytic lymphohistiocytosis. (For schematic purposes the circles in the Venn diagram have been scaled to PubMed citations.)
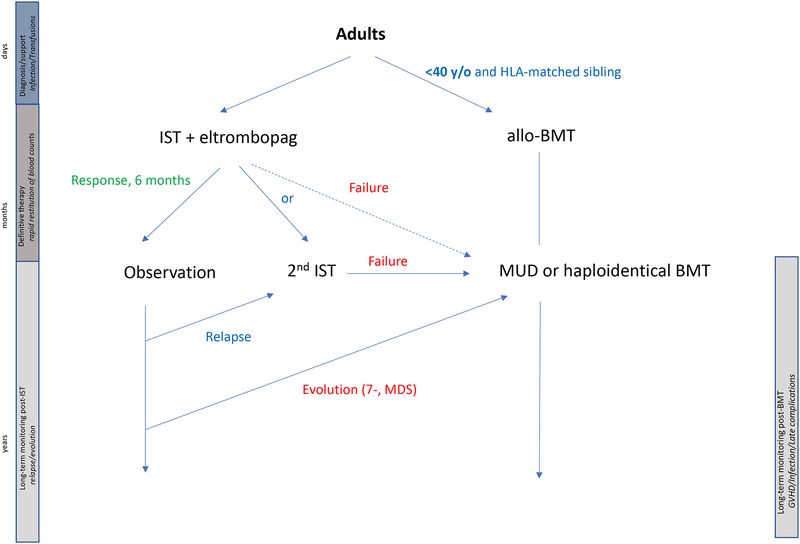
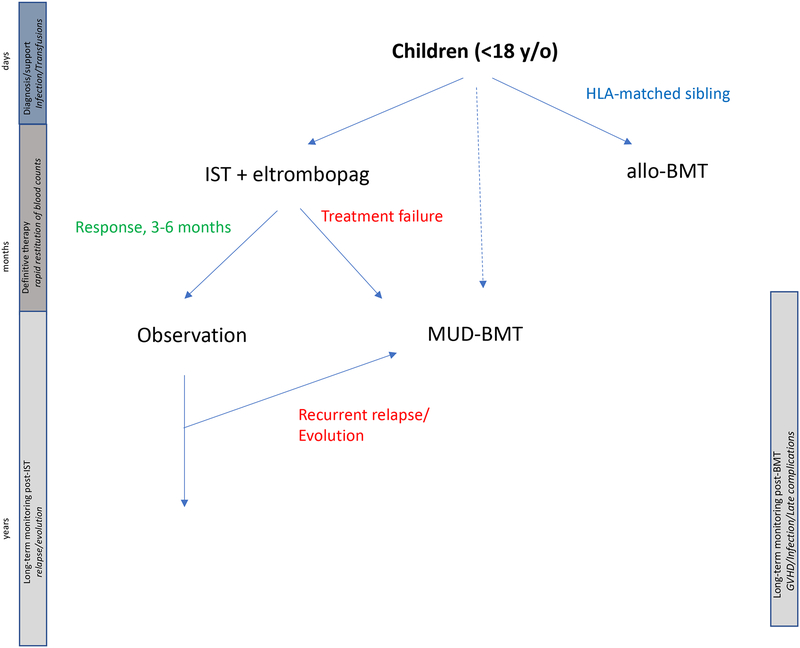
Treatment algorithms for A) children and B) adults with immune aplastic anemia. Treatment strategies are not fixed, due to developing results, especially long-term, with the use of new agents like eltrombopag and transplants from alternative donors; proposed approaches are indicated with dashed arrows. The ordinate bars represent the stages of treatment: days to diagnose and stabilize the severely pancytopenic patient; months to select, implement, and complete definitive therapy; and years of monitoring for responses and complications. The ability to salvage the extremely susceptible neutropenic patient is fundamental to long-term outcomes. Undesirable delays from diagnosis to transplant should be avoidable when outcomes from immunosuppression are clear in 3–6 months. Patients who fail immunosuppression, or who develop complications can do well with second-line transplant. IST=immunosuppression, BMT= bone marrow transplantation, MUD=matched unrelated donor transplant.
Treatment algorithms for A) children and B) adults with immune aplastic anemia. Treatment strategies are not fixed, due to developing results, especially long-term, with the use of new agents like eltrombopag and transplants from alternative donors; proposed approaches are indicated with dashed arrows. The ordinate bars represent the stages of treatment: days to diagnose and stabilize the severely pancytopenic patient; months to select, implement, and complete definitive therapy; and years of monitoring for responses and complications. The ability to salvage the extremely susceptible neutropenic patient is fundamental to long-term outcomes. Undesirable delays from diagnosis to transplant should be avoidable when outcomes from immunosuppression are clear in 3–6 months. Patients who fail immunosuppression, or who develop complications can do well with second-line transplant. IST=immunosuppression, BMT= bone marrow transplantation, MUD=matched unrelated donor transplant.
References
-
- Kaufman DW, Kelly JP, Levy M, Shapiro S. The Drug Etiology of Agranulocytosis and Aplastic Anemia. New York: Oxford; 1991.
-
- Yang C, Zhang X. Incidence survey of leukemia in China. Chinese Medical Sciences Journal 1991;6:65–70. - PubMed
-
- Gross SA, Irons RD, Schnatter AR, et al. A hospital-based case control study of aplastic anemia in Shanghai, China. Chem Biol Interact 2010;184:165–73. - PubMed
-
- Garaycoechea JI, Patel KJ. Why does the bone marrow fail in Fanconi anemia? Blood 2014;123:26–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical