

Effect of Intrathecal Baclofen on Pain and Quality of Life in Poststroke Spasticity
- PMID: 30354975
- PMCID: PMC6116794
- DOI: 10.1161/STROKEAHA.118.022255
Effect of Intrathecal Baclofen on Pain and Quality of Life in Poststroke Spasticity
Abstract
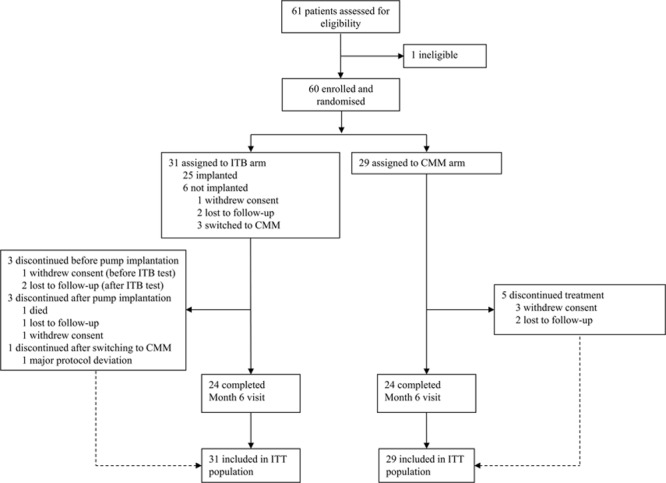
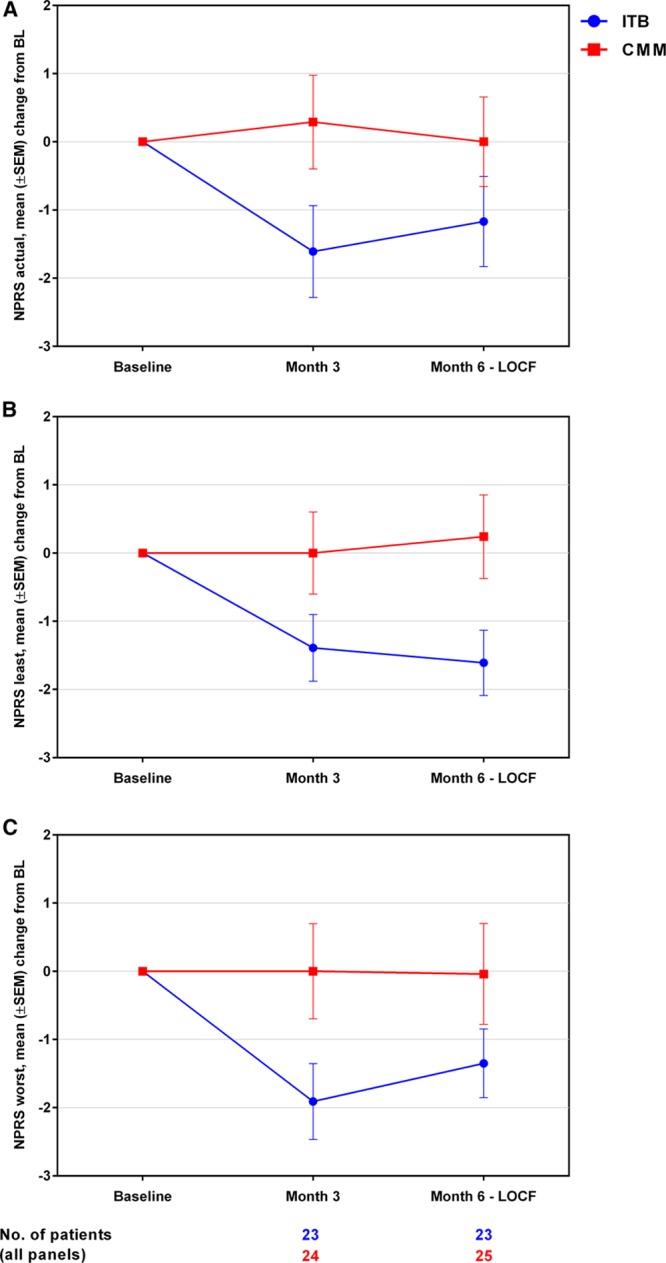
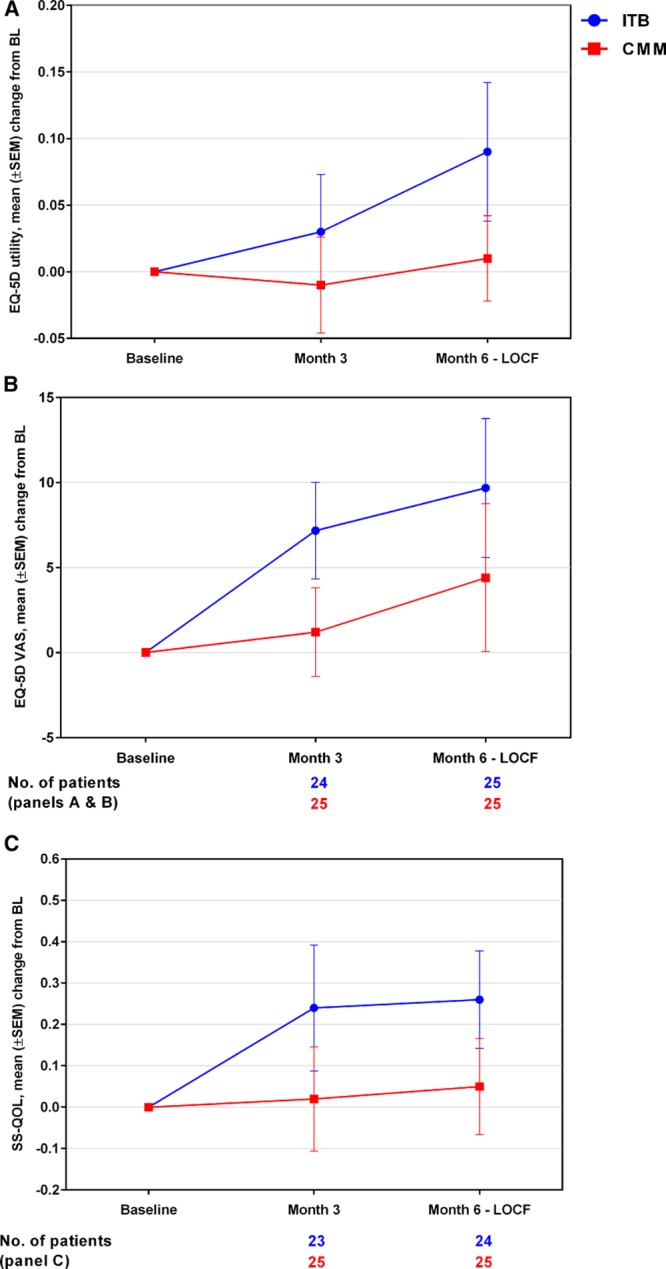
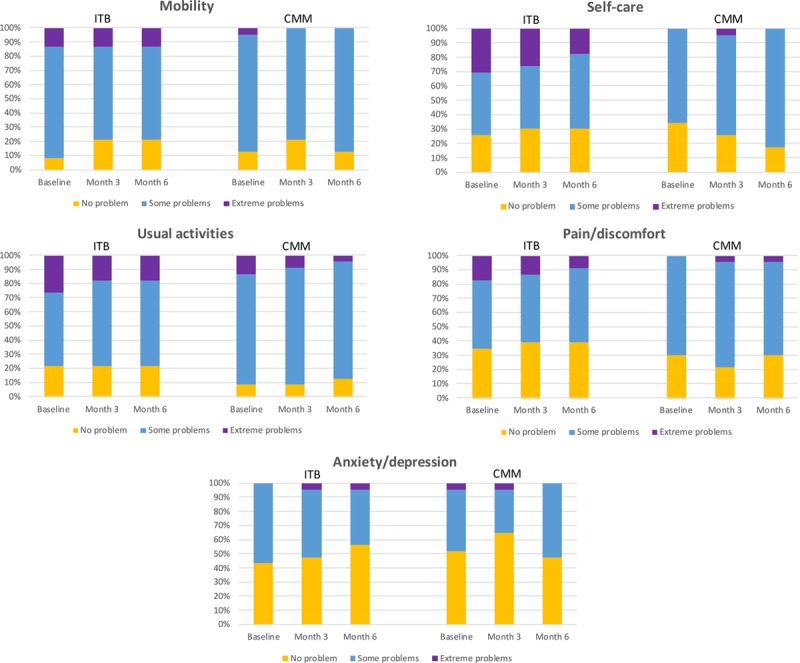
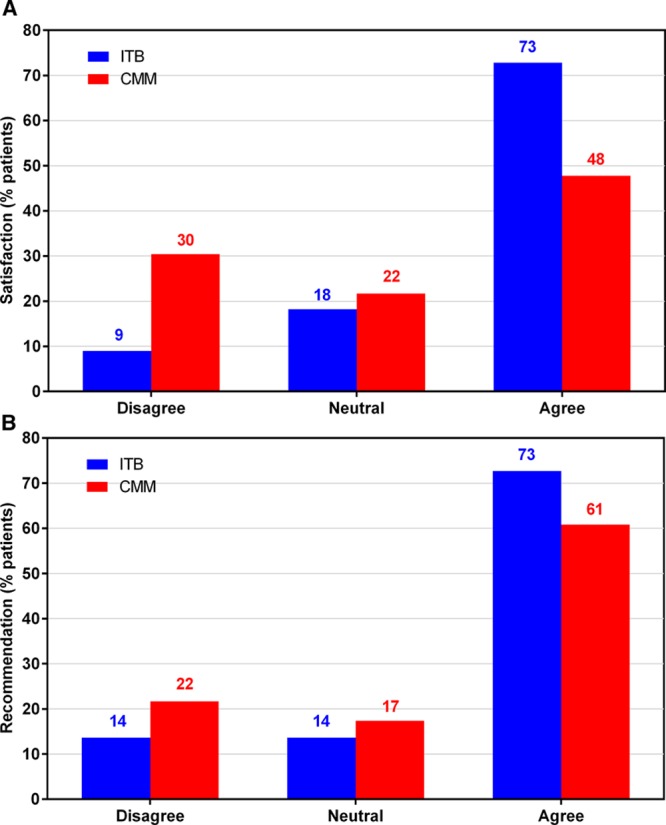
Background and Purpose- Intrathecal baclofen (ITB) is an effective treatment for managing patients with severe poststroke spasticity, who can experience continued pain and decline in their quality of life (QoL). SISTERS (Spasticity In Stroke-Randomized Study) was a randomized, controlled, open-label, multicenter, phase 4 study to evaluate ITB therapy versus conventional medical management (CMM) with oral antispastic medications for treatment of poststroke spasticity. Methods- Poststroke patients with spasticity in ≥2 extremities and an Ashworth Scale score of ≥3 in ≥2 affected lower extremity muscle groups were randomized (1:1) to ITB (N=31) or CMM (N=29). Both treatment arms received physiotherapy throughout. The primary outcome was the change in average Ashworth Scale score in the lower extremities of the affected side from baseline to month 6. Here, we report results for secondary outcomes: pain via the Numeric Pain Rating Scale, health-related QoL by the EuroQol-5 dimensional 3 level utility score and health status visual analog scale score, stroke-specific QoL, and patient satisfaction. Analyses were performed on an intention-to-treat basis. Results- We observed significant treatment effects in favor of ITB over CMM for changes from baseline to month 6 in Numeric Pain Rating Scale scores for actual pain (ITB versus CMM: mean, -1.17 [SD, 3.17] versus 0.00 [3.29]; median, -1.00 versus 0.00; P=0.0380) and least pain (mean, -1.61 [2.29] versus 0.24 [3.07]; median, -1.00 versus 0.00; P=0.0136), and EuroQol-5 dimensional 3 level utility scores (mean, +0.09 [0.26] versus +0.01 [0.16]; median, +0.07 versus 0.00; P=0.0197). Between-group differences were not statistically significant for EuroQol-5 dimensional 3 level visual analog scale, stroke-specific QoL summary, or Numeric Pain Rating Scale worst pain scores, although ITB patients showed greater numeric improvements from baseline during follow-up. More ITB patients than CMM patients (73% versus 48%) were satisfied with the spasticity reduction at month 6. Conclusions- These data support that ITB therapy is associated with improvements in pain and QoL in poststroke patients. Clinical Trial Registration- URL: https://www.clinicaltrials.gov . Unique identifier: NCT01032239.
Keywords: baclofen; muscle spasticity; pain; quality of life; stroke.
Figures
References
-
- Wissel J, Manack A, Brainin M. Toward an epidemiology of poststroke spasticity. Neurology. 2013;80(3)(suppl 2):S13–S19. doi: 10.1212/WNL.0b013e3182762448. - PubMed
-
- Dvorak EM, Ketchum NC, McGuire JR. The underutilization of intrathecal baclofen in poststroke spasticity. Top Stroke Rehabil. 2011;18:195–202. doi: 10.1310/tsr1803-195. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
