

Effect of Intracoronary Metformin on Myocardial Infarct Size in Swine
- PMID: 30355033
- PMCID: PMC6207210
- DOI: 10.1161/CIRCRESAHA.118.313341
Effect of Intracoronary Metformin on Myocardial Infarct Size in Swine
Abstract
Rationale: Metformin has been demonstrated to decrease infarct size (IS) and prevent postinfarction left ventricular (LV) remodeling in rodents when given intravenously at the time of reperfusion. It remains unclear whether similar cardioprotection can be achieved in a large animal model.
Objective: The objective of this study was to determine whether intravascular infusion of metformin at the time of reperfusion reduces myocardial IS in a porcine model of acute myocardial infarction.
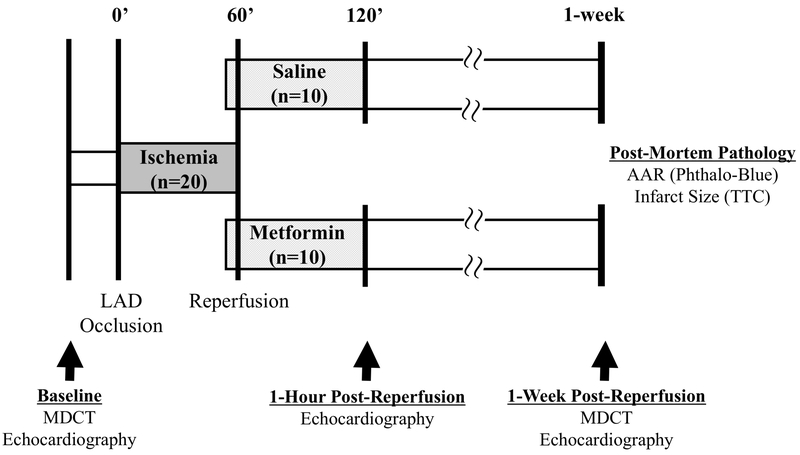
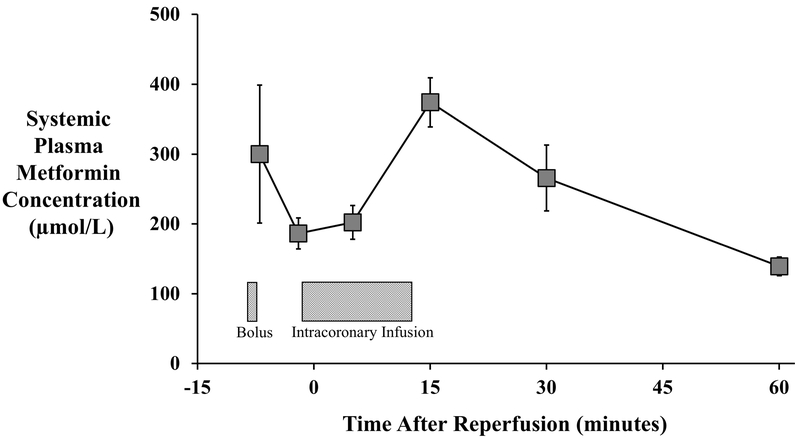
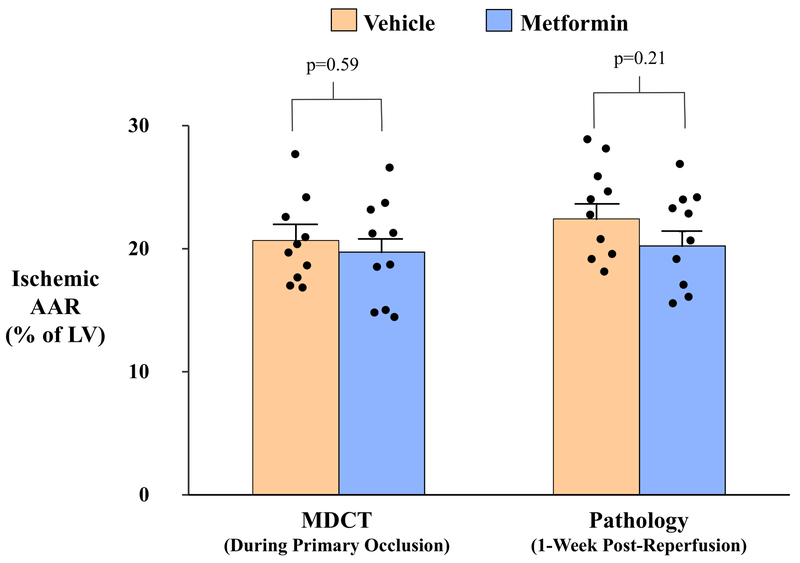
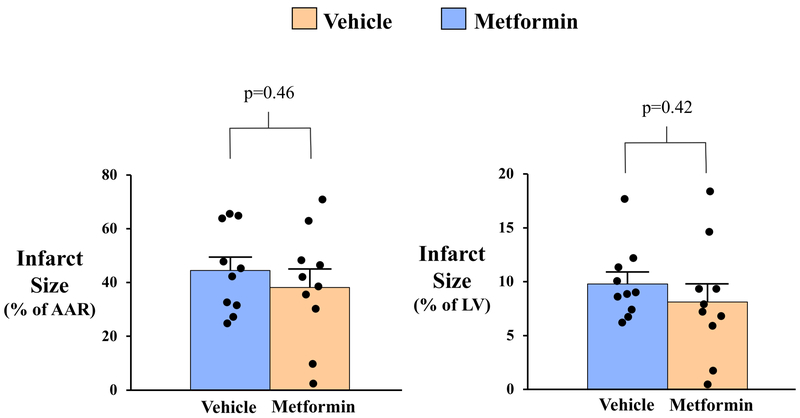
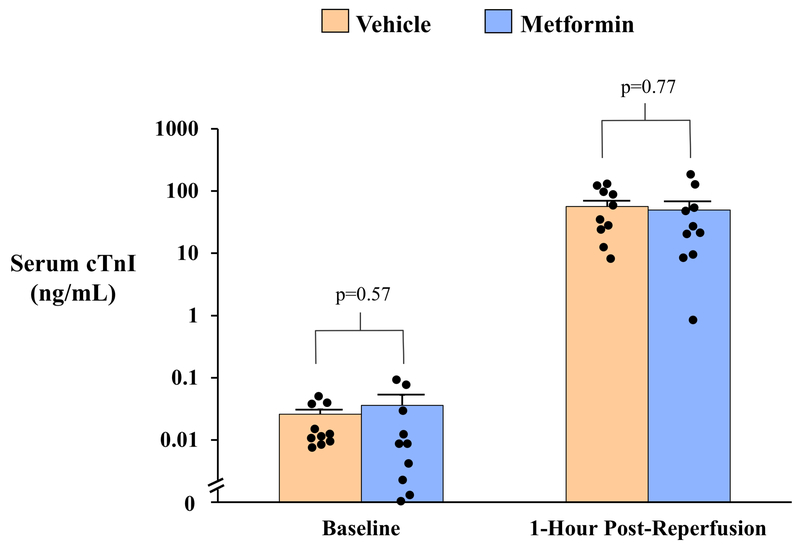
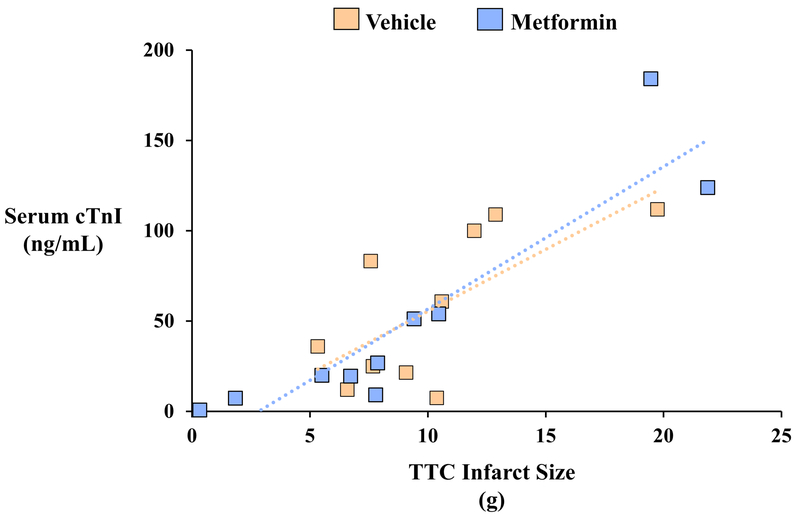
Methods and results: In a blinded and randomized preclinical study, closed-chest swine (n=20) were subjected to a 60-minute left anterior descending coronary artery occlusion to produce myocardial infarction. Contrast-enhanced computed tomography was performed during left anterior descending coronary artery occlusion to assess the ischemic area-at-risk. Animals were randomized to receive either metformin or vehicle as an initial intravenous bolus (5 mg/kg) 8 minutes before reperfusion, followed by a 15-minute left coronary artery infusion (1 mg/kg per minute) commencing with the onset of reperfusion. Echocardiography and computed tomographic imaging of LV function were performed 1 week later, at which time the heart was removed for postmortem pathological analysis of area-at-risk and IS (triphenyltetrazolium chloride). Baseline variables including hemodynamics and LV function were similar between groups. Peak circulating metformin concentrations of 374±35 µmol/L were achieved 15 minutes after reperfusion. There was no difference between the area-at-risk as a percent of LV mass by computed tomography (vehicle: 20.7%±1.1% versus metformin: 19.7%±1.3%; P=0.59) or postmortem pathology (22.4%±1.2% versus 20.2%±1.2%; P=0.21). IS relative to area-at-risk averaged 44.5%±5.0% in vehicle-treated versus 38.2%±6.8% in metformin-treated animals ( P=0.46). There was no difference in global function 7 days after myocardial infarction as assessed by echocardiography or computed tomographic ejection fraction (56.2%±2.6% versus 56.3%±2.4%; P=0.98).
Conclusions: In contrast to rodent hearts, postconditioning with high-dose metformin administered immediately before reperfusion does not reduce IS or improve LV function 7 days after myocardial infarction in swine. These results reinforce the importance of rigorously testing therapies in large animal models to facilitate clinical translation of novel cardioprotective therapies.
Keywords: infarction; metformin; models, animal; myocardial infarction; ventricular remodeling.
Figures


Comment in
-
Translation, Translation, Translation.Circ Res. 2018 Sep 28;123(8):931-933. doi: 10.1161/CIRCRESAHA.118.313947. Circ Res. 2018. PMID: 30355042 No abstract available.
References
-
- Heusch G and Gersh BJ. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: a continual challenge. EurHeart J. 2017;38:774–784. - PubMed
-
- Heusch G Molecular basis of cardioprotection: signal transduction in ischemic pre-, post-, and remote conditioning. Circ Res. 2015;116:674–99. - PubMed
-
- Varjabedian L, Bourji M, Pourafkari L and Nader ND Cardioprotection by Metformin: Beneficial Effects Beyond Glucose Reduction. Am J Cardiovasc Drugs. 2018. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
