

Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk
- PMID: 30355075
- PMCID: PMC6205735
- DOI: 10.1161/CIRCRESAHA.118.312806
Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk
Abstract
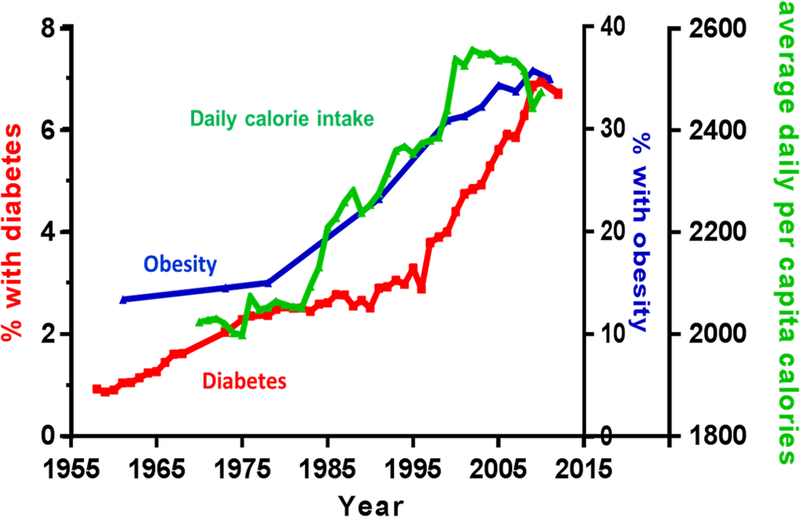
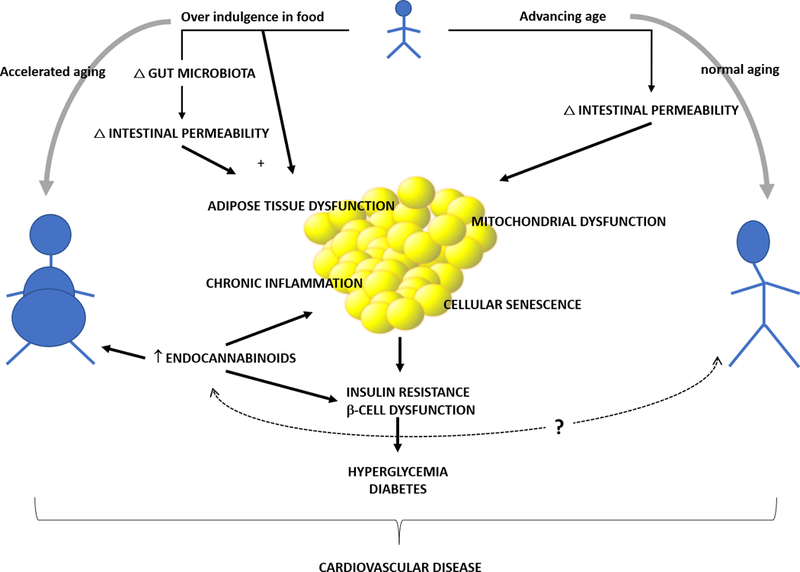
Aging and diabetes mellitus are 2 well-known risk factors for cardiovascular disease (CVD). During the past 50 years, there has been an dramatic increase in life expectancy with a simultaneous increase in the prevalence of diabetes mellitus in the older population. This large number of older individuals with diabetes mellitus is problematic given that CVD risk associated with aging and diabetes mellitus. In this review, we summarize epidemiological data relating to diabetes mellitus and CVD, with an emphasis on the aging population. We then present data on hyperglycemia as a risk factor for CVD and review the current knowledge of age-related changes in glucose metabolism. Next, we review the role of obesity in the pathogenesis of age-related glucose dysregulation, followed by a summary of the results from major randomized controlled trials that focus on cardiovascular risk reduction through glycemic control, with a special emphasis on older adults. We then conclude with our proposed model of aging that body composition changes and insulin resistance link possible dysregulation of physiological pathways leading to obesity and diabetes mellitus-both forms of accelerated aging-and risks for CVD.
Keywords: aging; cardiovascular diseases; diabetes mellitus; obesity; risk factors.
Figures
References
-
- West LA, Cole S, Goodkind D and He W. 65+ in the United States: 2010. 2014.
-
- He W, Goodkind D and Kowal P. An Aging World: 2015; International Population Reports. 2016.
-
- Savji N, Rockman CB, Skolnick AH, Guo Y, Adelman MA, Riles T and Berger JS. Association between advanced age and vascular disease in different arterial territories: a population database of over 3.6 million subjects. Journal of the American College of Cardiology. 2013;61:1736–43. - PubMed
-
- Centers for Disease Control and Prevention. Long-term Trends in Diabetes, 2017 Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services; 2017 2017.
-
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017 Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services; 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
