

Long-Term Consequences of Worsened Poststroke Status in Patients With Premorbid Disability
- PMID: 30355105
- PMCID: PMC6159688
- DOI: 10.1161/STROKEAHA.118.022416
Long-Term Consequences of Worsened Poststroke Status in Patients With Premorbid Disability
Abstract
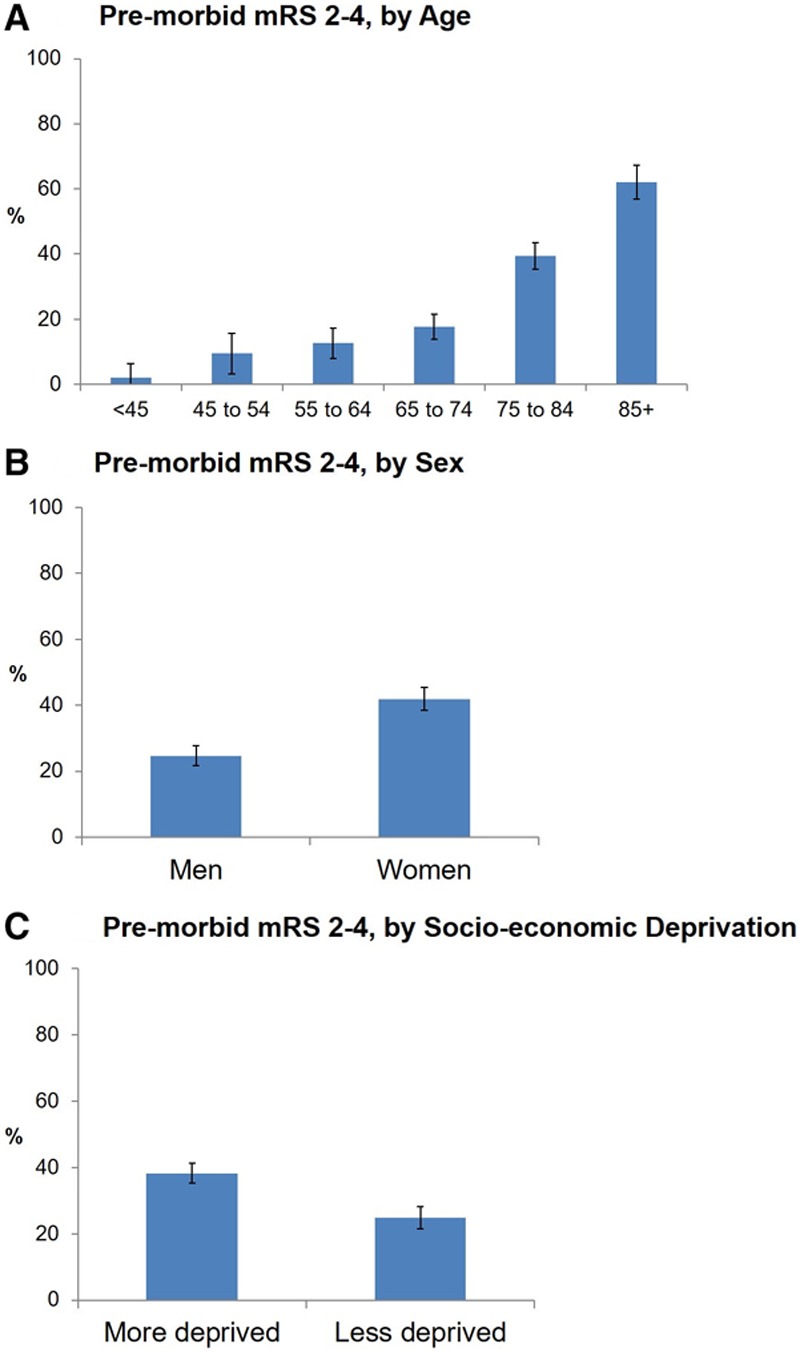
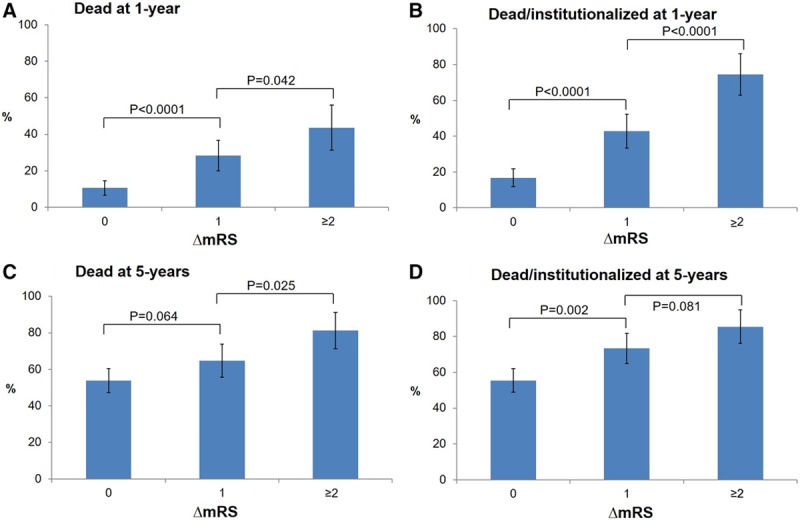
Background and Purpose- Patients with premorbid disability, generally defined as modified Rankin Scale (mRS) score ≥2, are often excluded from trials of acute stroke therapies. However, increased disability in such patients will adversely affect long-term outcomes if treatments are withheld in routine practice. We assessed the extent to which increased disability poststroke influences 5-year mortality, institutionalization, and costs in premorbidly disabled patients. Methods- In a population-based, prospective cohort of patients with ischemic stroke (OXVASC [Oxford Vascular Study], 2002-2014), we tracked mortality, institutionalization, and healthcare/social-care costs during follow-up. We compared 5-year mortality and poststroke institutionalization (Cox regressions) and 5-year healthcare/social-care costs (generalized linear model) in 3-month survivors with premorbid mRS of 2 to 4 (excluding extreme disability, mRS=5), based on the degree of change in mRS(ΔmRS) from prestroke to 3 months poststroke, adjusting analyses for age/sex/initial National Institutes of Health Stroke Scale. Results- Among 1607 patients, 530 (33.0%) had premorbid mRS of 2 to 4. Only 2 premorbidly disabled patients received thrombolysis, but 421 (79.4%) were alive at 3 months. ΔmRS was independently associated with 5-year mortality/institutionalization (adjusted hazard ratio for ΔmRS=1 versus 0: 1.59; 95% CI, 1.20-2.11; ΔmRS=2: 2.39; 95% CI, 1.62-3.53; ΔmRS=3: 4.12; 95% CI, 1.98-8.60; P<0.001) and costs (margin for ΔmRS ≥2 versus 0: $30 011, 95% CI, $4222-55 801; P=0.023). Results were similar on examining patients with premorbid mRS of 2, 3, and 4 separately (eg, 5-year mortality/institutionalization adjusted hazard ratio for premorbid mRS=3 with ΔmRS=1 versus 0: 1.60; 95% CI, 1.06-2.42; P=0.027; ΔmRS=2: 3.20; 95% CI, 1.85-5.54; P<0.001). Conclusions- Patients with stroke with premorbid disability have higher mortality, institutionalization, and costs if they accumulate additional disability because of the stroke. These findings highlight the long-term outcomes expected if acute interventions are routinely withheld in patients with mild-moderate premorbid disability and suggest that trials/registries should include such patients.
Keywords: cerebrovascular; cohort studies; disorders; humans; prognosis; survivors.
Figures
References
-
- Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E, et al. Stroke Thrombolysis Trialists’ Collaborative Group. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384:1929–1935. doi: 10.1016/S0140-6736(14)60584-5. - PMC - PubMed
-
- Goyal M, Menon BK, van Zwam WH, Dippel DW, Mitchell PJ, Demchuk AM, et al. HERMES Collaborators. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387:1723–1731. doi: 10.1016/S0140-6736(16)00163-X. - PubMed
-
- Cappellari M, Bosco M, Forlivesi S, Tomelleri G, Micheletti N, Carletti M, et al. Reasons for exclusion from intravenous thrombolysis in stroke patients admitted to the stroke unit. J Thromb Thrombolysis. 2016;42:593–599. doi: 10.1007/s11239-016-1406-8. - PubMed
-
- Kwok CS, Clark A, Ford GA, Durairaj R, Dixit AK, Davis J, et al. Association between prestroke disability and inpatient mortality and length of acute hospital stay after acute stroke. J Am Geriatr Soc. 2012;60:726–732. doi: 10.1111/j.1532-5415.2011.03889.x. - PubMed
-
- Abdul-Rahim AH, Quinn TJ, Alder S, Clark AB, Musgrave SD, Langhorne P, et al. Derivation and validation of a novel prognostic scale (modified-stroke subtype, oxfordshire community stroke project classification, age, and prestroke modified Rankin) to predict early mortality in acute stroke. Stroke. 2016;47:74–79. doi: 10.1161/STROKEAHA.115.009898. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
