

Pathology and Pathogenesis of Chagas Heart Disease
- PMID: 30355152
- PMCID: PMC7373119
- DOI: 10.1146/annurev-pathol-020117-043711
Pathology and Pathogenesis of Chagas Heart Disease
Abstract
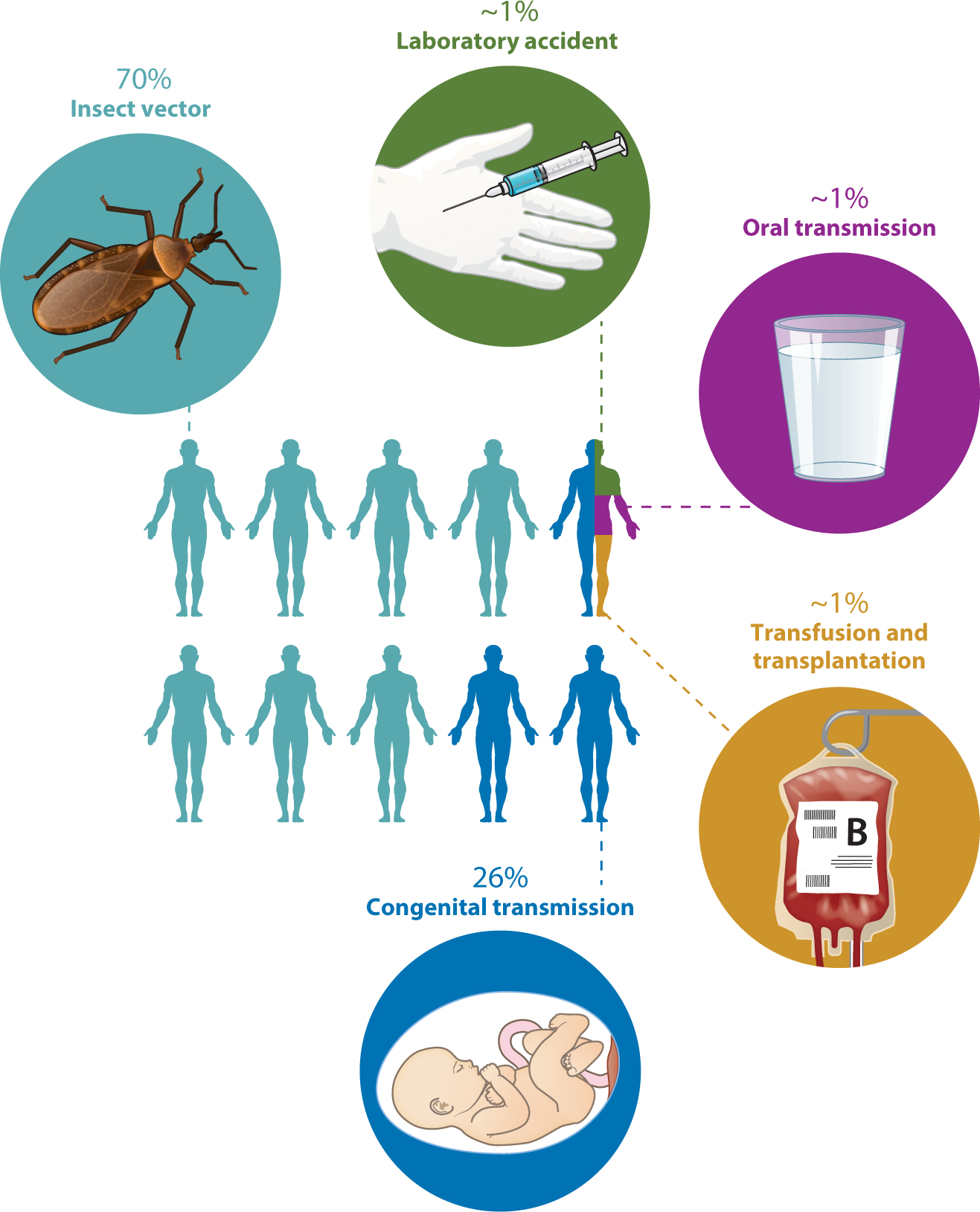
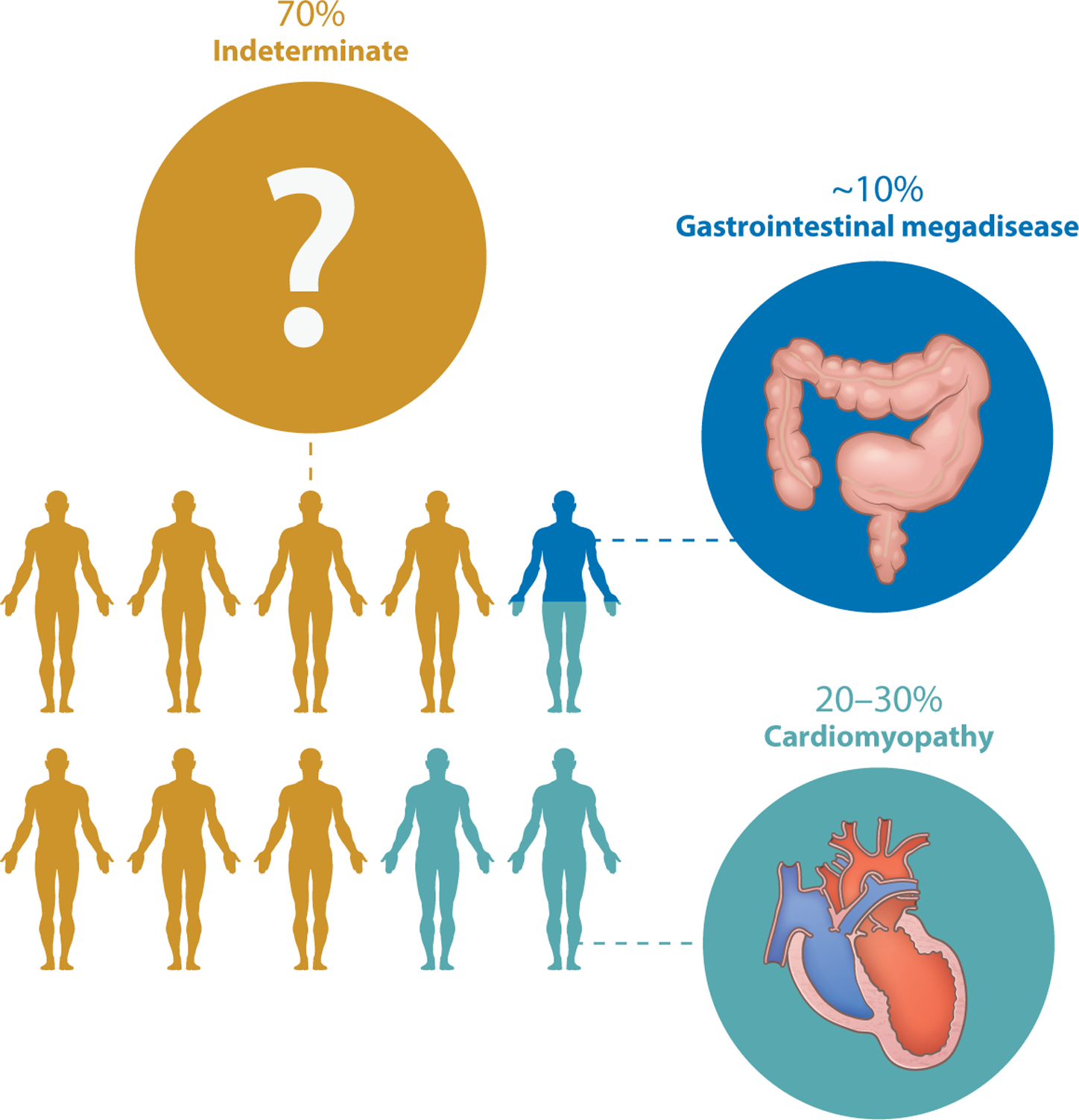
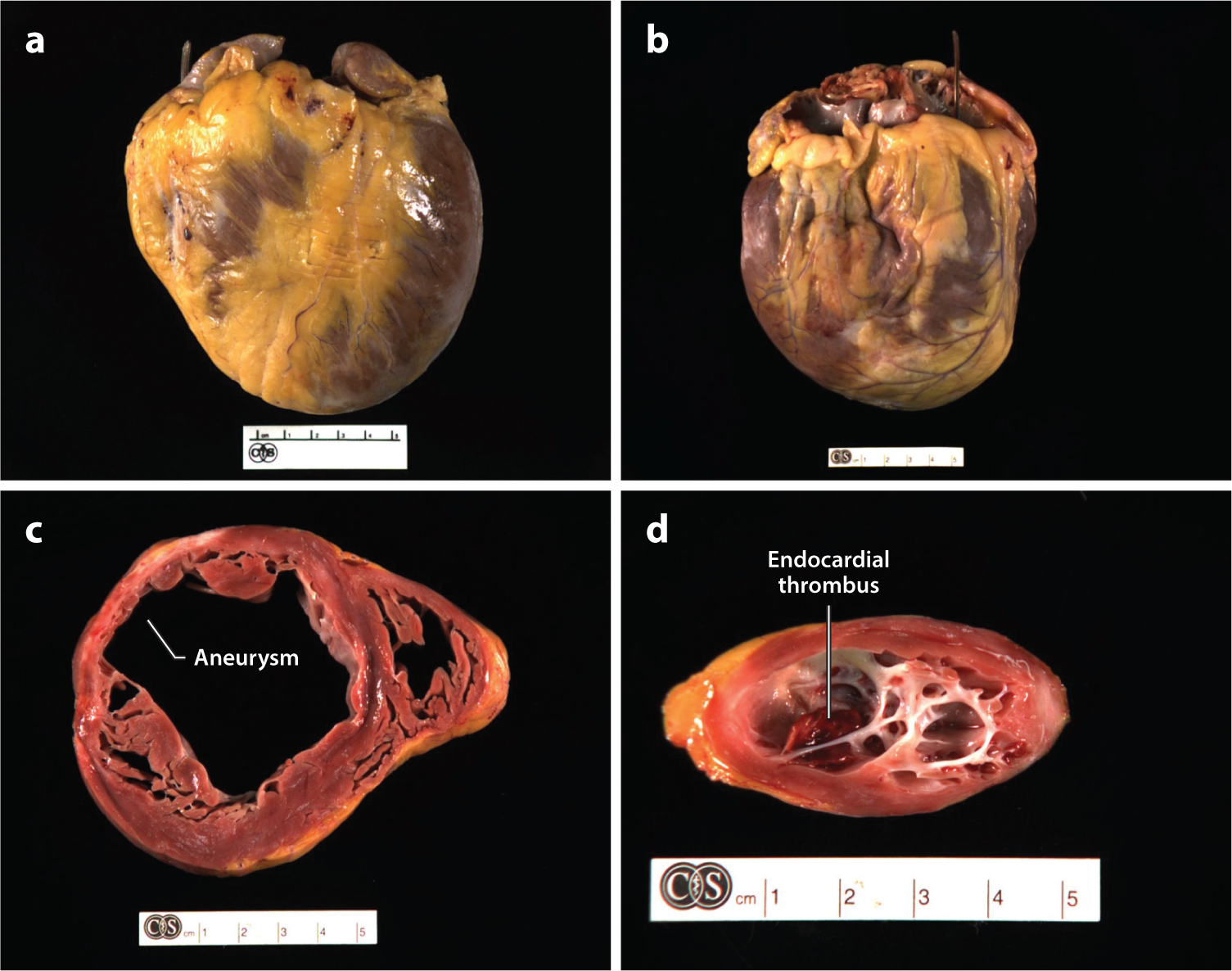
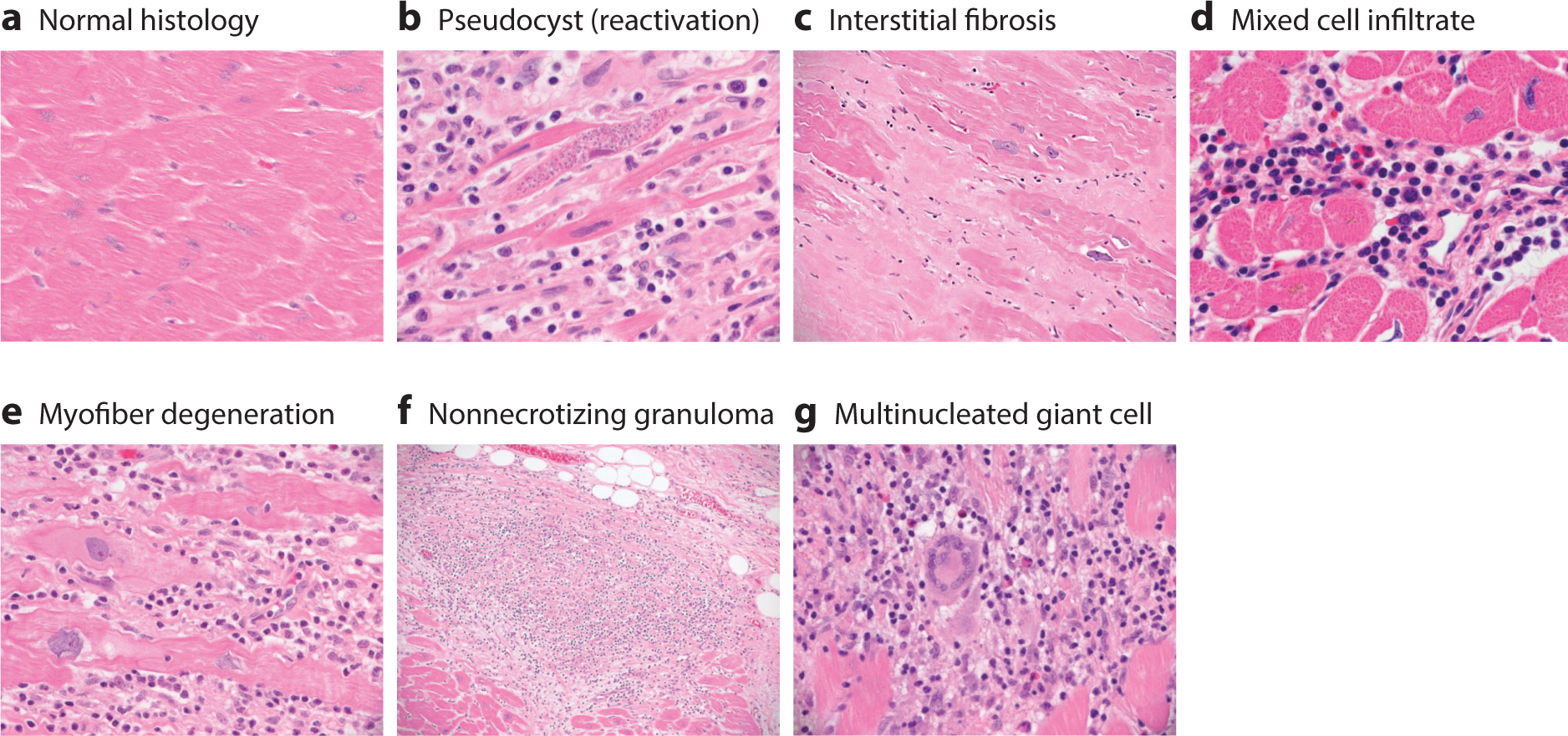
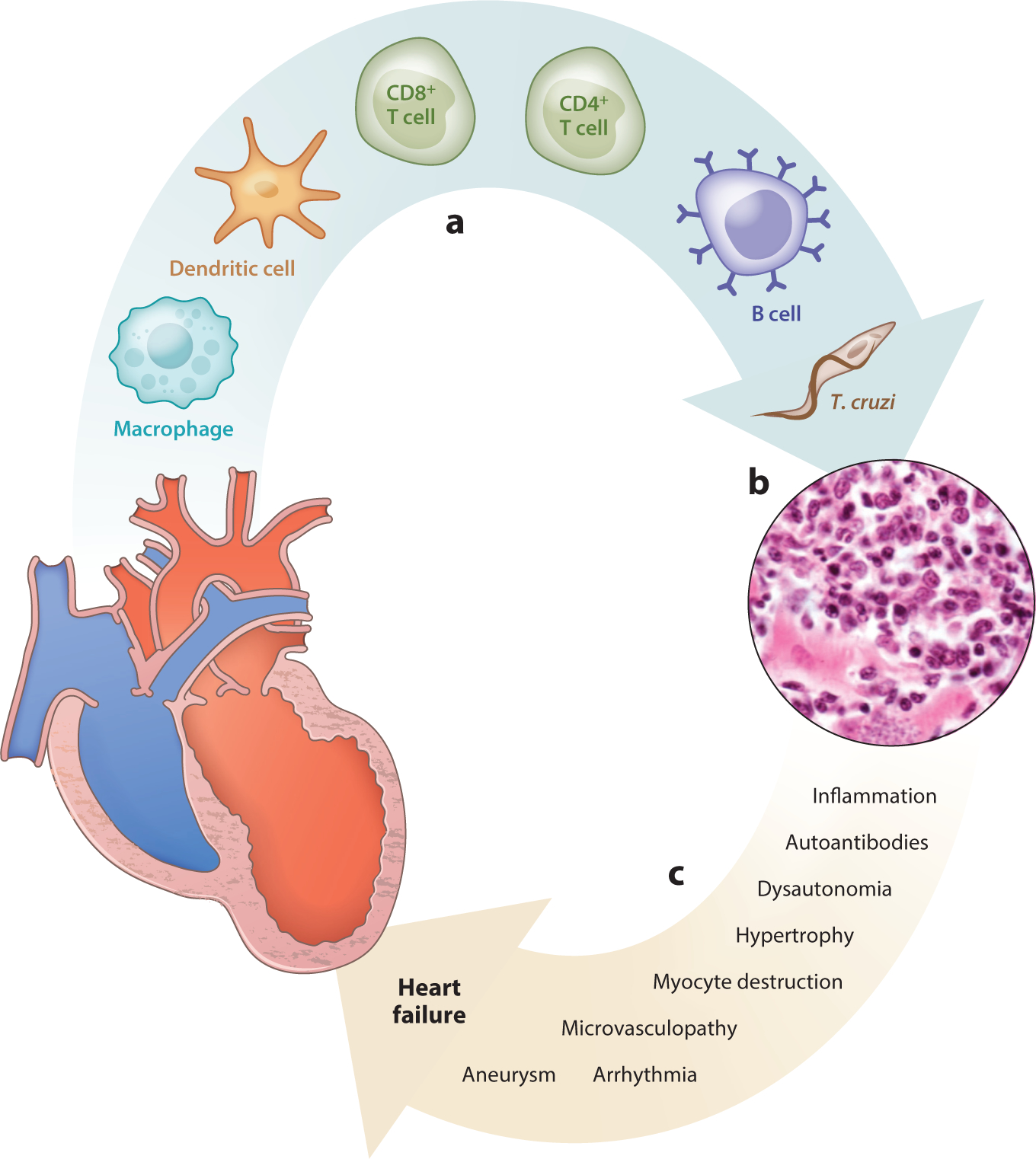
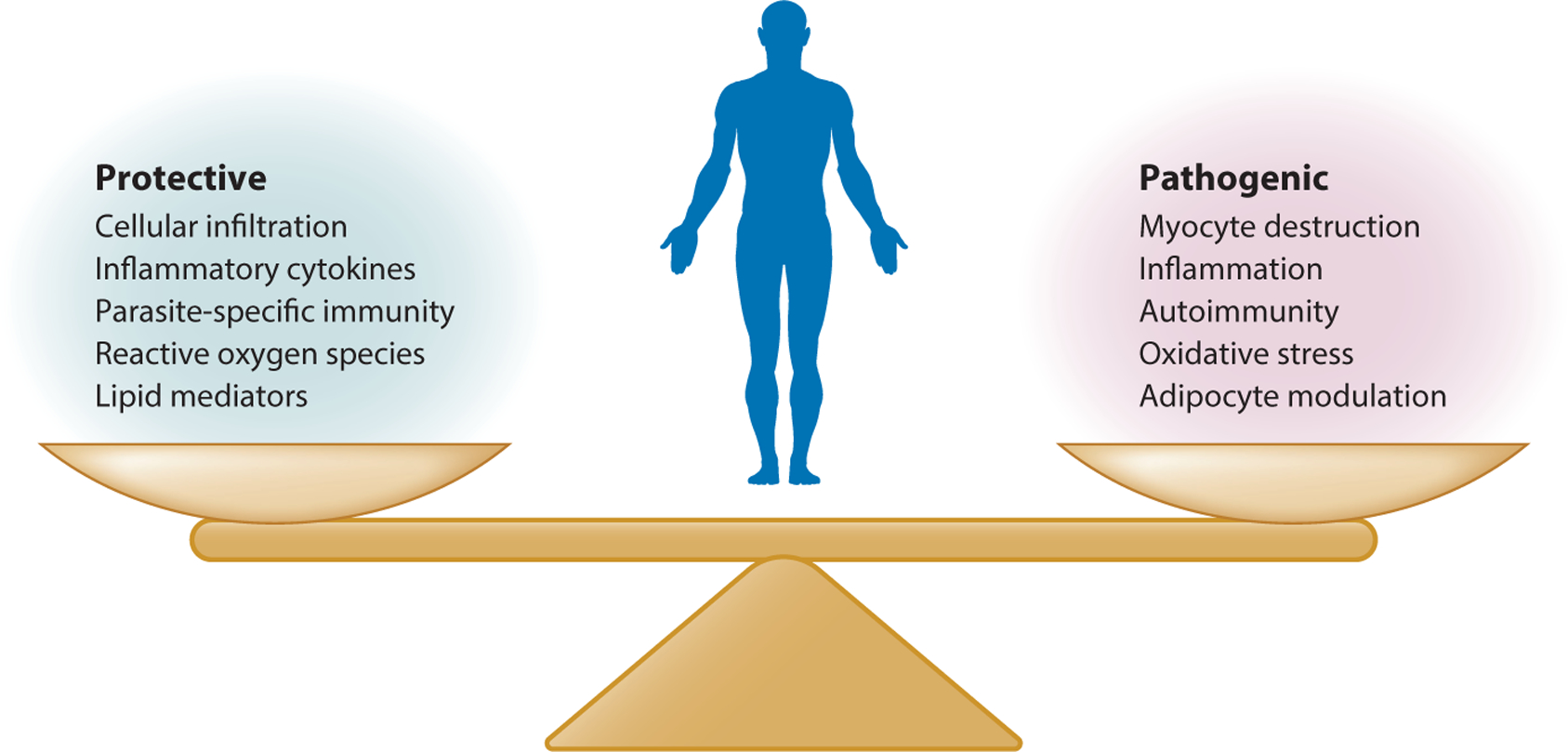
Chagas heart disease is an inflammatory cardiomyopathy that develops in approximately one-third of people infected with the protozoan parasite Trypanosoma cruzi. One way T. cruzi is transmitted to people is through contact with infected kissing bugs, which are found in much of the Western Hemisphere, including in vast areas of the United States. The epidemiology of T. cruzi and Chagas heart disease and the varied mechanisms leading to myocyte destruction, mononuclear cell infiltration, fibrosis, and edema in the heart have been extensively studied by hundreds of scientists for more than 100 years. Despite this wealth of knowledge, it is still impossible to predict what will happen in an individual infected with T. cruzi because of the tremendous variability in clonal parasite virulence and human susceptibility to infection and the lack of definitive molecular predictors of outcome from either side of the host-parasite equation. Further, while several distinct mechanisms of pathogenesis have been studied in isolation, it is certain that multiple coincident mechanisms combine to determine the ultimate outcome. For these reasons, Chagas disease is best considered a collection of related but distinct illnesses. This review highlights the pathology and pathogenesis of the most common adverse sequela of T. cruzi infection-Chagas heart disease-and concludes with a discussion of key unanswered questions and a view to the future.
Keywords: Chagas; cardiomyopathy; heart; myocarditis; pathogenesis; trypanosome.
Figures
References
-
- Brener Z 1973. Biology of Trypanosoma cruzi. Annu. Rev. Microbiol 27:347–82 - PubMed
-
- WHO (World Health Organ.). 2002. Control of Chagas Disease: Second Report of the WHO Expert Committee. Geneva, Switzerland: WHO
-
- Shikanai-Yasuda MA, Carvalho NB. 2012. Oral transmission of Chagas disease. Clin. Infect. Dis 54:845–52 - PubMed
-
- PAHO (Pan Am. Health Organ.). 2018. Chagas disease portal. Pan Am. Health Organ http://www.paho.org/hq/index.php?option=com_topics&view=article&id=10&It...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
