

Immediate and Delayed Procedural Stroke or Death in Stenting Versus Endarterectomy for Symptomatic Carotid Stenosis
- PMID: 30355202
- PMCID: PMC6209445
- DOI: 10.1161/STROKEAHA.118.020684
Immediate and Delayed Procedural Stroke or Death in Stenting Versus Endarterectomy for Symptomatic Carotid Stenosis
Abstract
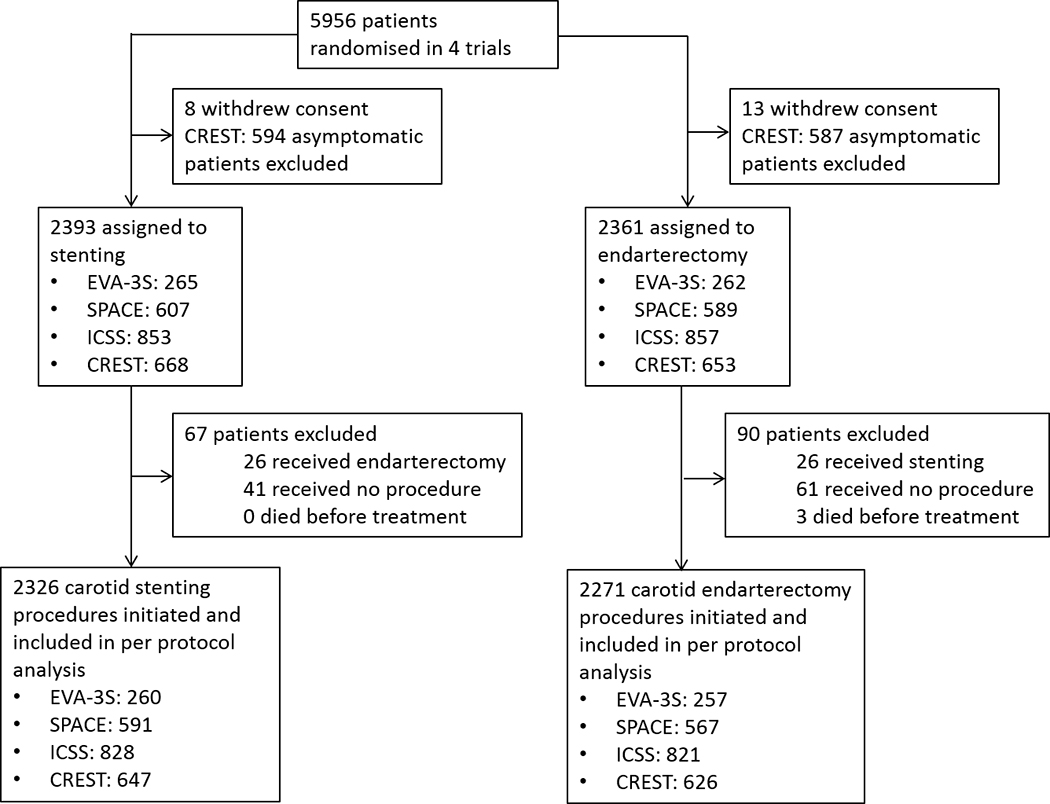
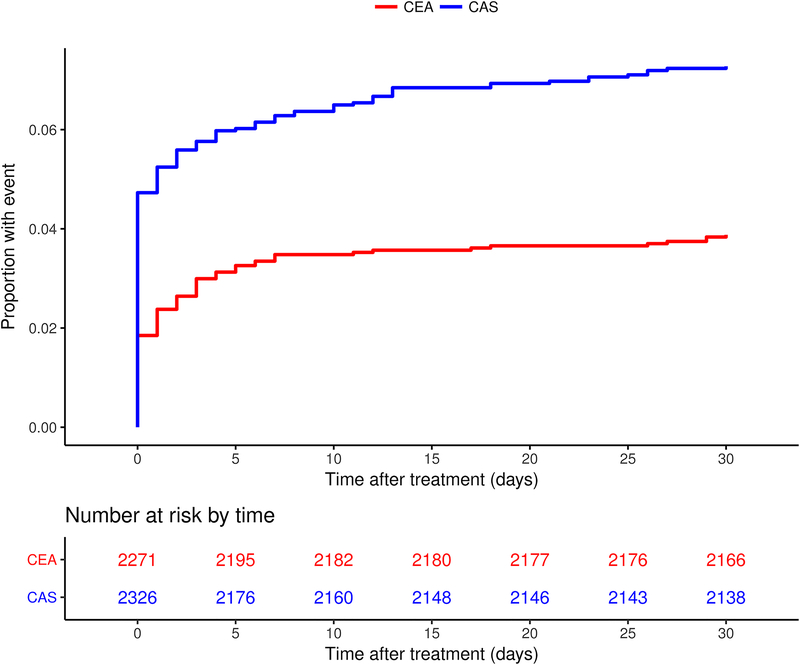
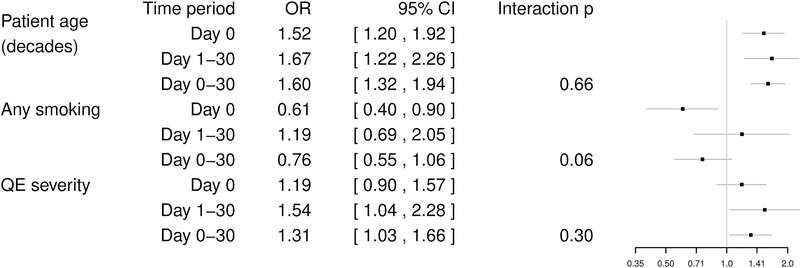
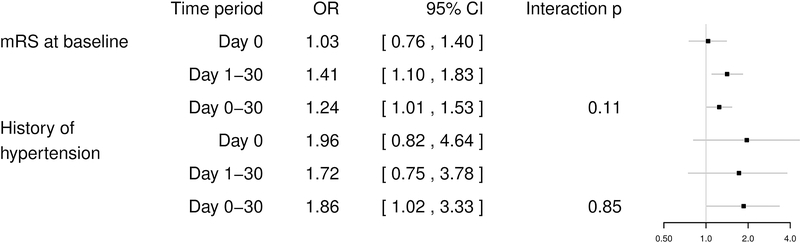
Background and Purpose- Stenting for symptomatic carotid stenosis (carotid artery stenting [CAS]) carries a higher risk of procedural stroke or death than carotid endarterectomy (CEA). It is unclear whether this extra risk is present both on the day of procedure and within 1 to 30 days thereafter and whether clinical risk factors differ between these periods. Methods- We analyzed the risk of stroke or death occurring on the day of procedure (immediate procedural events) and within 1 to 30 days thereafter (delayed procedural events) in 4597 individual patients with symptomatic carotid stenosis who underwent CAS (n=2326) or CEA (n=2271) in 4 randomized trials. Results- Compared with CEA, patients treated with CAS were at greater risk for immediate procedural events (110 versus 42; 4.7% versus 1.9%; odds ratio, 2.6; 95% CI, 1.9-3.8) but not for delayed procedural events (59 versus 46; 2.5% versus 2.0%; odds ratio, 1.3; 95% CI, 0.9-1.9; interaction P=0.006). In patients treated with CAS, age increased the risk for both immediate and delayed events while qualifying event severity only increased the risk of delayed events. In patients treated with CEA, we found no risk factors for immediate events while a higher level of disability at baseline and known history of hypertension were associated with delayed procedural events. Conclusions- The increased procedural stroke or death risk associated with CAS compared with CEA was caused by an excess of events occurring on the day of procedure. This finding demonstrates the need to enhance the procedural safety of CAS by technical improvements of the procedure and increased operator skill. Higher age increased the risk for both immediate and delayed procedural events in CAS, mechanisms of which remain to be elucidated. Clinical Trial Registration- URL: https://clinicaltrials.gov . Unique identifier: NCT00190398. URL: http://www.isrctn.com . Unique identifier: ISRCTN57874028. URL: http://www.isrctn.com . Unique identifier: ISRCTN25337470. URL: https://clinicaltrials.gov . Unique identifier: NCT00004732.
Keywords: carotid stenosis; endarterectomy; risk; stents; stroke.
Conflict of interest statement
Disclosures
LHB has received an unrestricted research grant from AstraZeneca, as well as consultancy and advisory board fees from Amgen, Bayer, Bristol-Myers Squibb, and Claret Medical. PR has received lecture fees and advisory board fees from Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Covidien, and Pfizer. OJ received speaker fees from Medtronic, Stryker and Philips. All other authors declare no competing interests.
Figures
References
-
- Carotid Stenting Trialists Collaboration, Bonati LH, Dobson J, Algra A, Branchereau A, Chatellier G, et al. Short-term outcome after stenting versus endarterectomy for symptomatic carotid stenosis: A preplanned meta-analysis of individual patient data. Lancet. 2010;376:1062–1073 - PubMed
-
- Howard G, Roubin GS, Jansen O, Hendrikse J, Halliday A, Fraedrich G, et al. Association between age and risk of stroke or death from carotid endarterectomy and carotid stenting: A meta-analysis of pooled patient data from four randomised trials. Lancet. 2016;387:1305–1311 - PubMed
-
- Mas JL, Arquizan C, Calvet D, Viguier A, Albucher JF, Piquet P, et al. Long-term follow-up study of endarterectomy versus angioplasty in patients with symptomatic severe carotid stenosis trial. Stroke. 2014;45:2750–2756 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
