

Laryngeal mask airway Unique™ position in paediatric patients undergoing magnetic resonance imaging (MRI): prospective observational study
- PMID: 30355285
- PMCID: PMC6201529
- DOI: 10.1186/s12871-018-0617-2
Laryngeal mask airway Unique™ position in paediatric patients undergoing magnetic resonance imaging (MRI): prospective observational study
Abstract
Background: Laryngeal mask UNIQUE® (LMAU) is supraglottic airway device with good clinical performance and low failure rate. Little is known about the ideal position of the LMAU on the magnetic resonance imaging (MRI) and whether radiological malposition can be associated with clinical performance (audible leak) in children. The primary aim of the study was to evaluate incidence of the radiologic malposition of the LMAU according to size. The secondary outcome was the clinical performance and associated complications (1st attempt success rate, audible leak) in LMAUs in correct position vs. radiologically misplaced LMAUs.
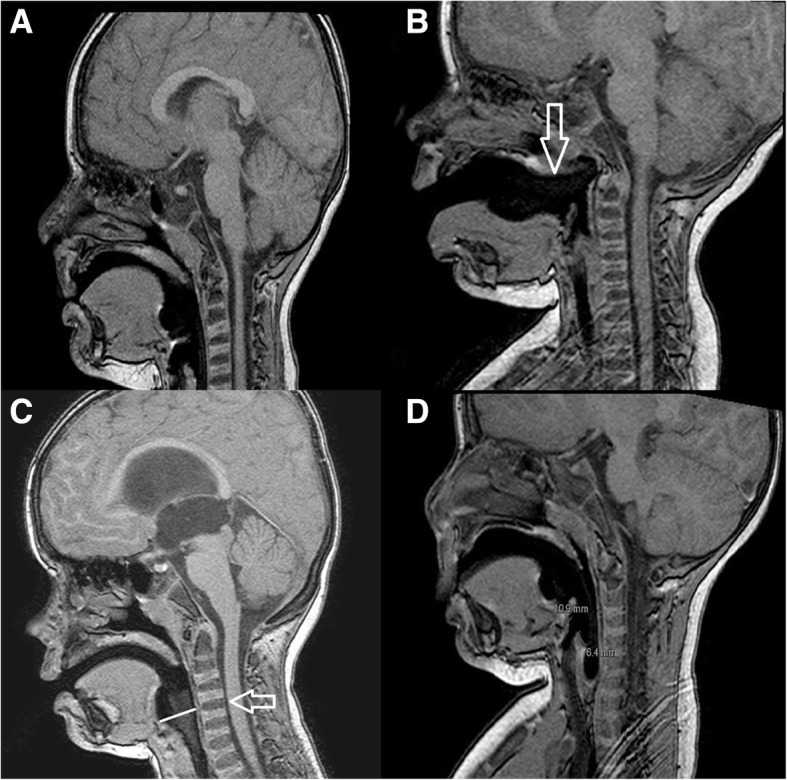
Methods: In prospective observational study, all paediatric patients undergoing MRI of the brain under general anaesthesia with the LMAU were included (1.9.2016-16.5.2017). The radiologically correct position: LMAU in hypopharynx, proximal cuff opposite to the C1 or C2 and distance A (proximal cuff end and aditus laryngis) ≤ distance B (distal cuff end and aditus laryngis). Malposition A: LMAU outside the hypopharynx. Malposition B: proximal cuff outside C1-C2. Malposition C: distance A ≥ distance B. We measured distances on the MRI image. Malposition incidence between LMAU sizes and first attempt success rate in trainees and consultant groups was compared using Fisher exact test, difference in incidence of malpositions using McNemar test and difference in leakage according to radiological position using two-sample binomial test.
Results: Overall 202 paediatric patients were included. The incidence of radiologically defined malposition was 26.2% (n = 53). Laryngeal mask was successfully inserted on the 1st attempt in 91.1% (n = 184) cases. Audible leak was detected in 3.5% (n = 7) patients. The radiologically defined malposition was present in 42.9% (n = 3) cases with audible leak. The rate of associated complications was 1.5% (n = 3): laryngospasm, desaturation, cough. In 4.0% (n = 8) the LMAU was soiled from blood. Higher incidence of radiological malposition was in LMAU 1.0, 1.5 and LMAU 3, 4 compared to LMAU 2 or LMAU 2.5 (p < 0.001).
Conclusion: Malposition was not associated with impaired clinical performance (audible leak, complications) of the LMAU or the need for alternative airway management.
Trial registration: Clinicaltrials.gov (NCT02940652) Registered 18 October 18 2016.
Keywords: Laryngeal mask; Magnetic resonance imaging; Paediatric anaesthesia; Position.
Conflict of interest statement
Ethics approval and consent to participate
Study was approved by Local Ethics Committee of University Hospital Brno, Czech Republic (9/2016) with waiver to obtain written informed consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
