

Adult height and risk of 50 diseases: a combined epidemiological and genetic analysis
- PMID: 30355295
- PMCID: PMC6201543
- DOI: 10.1186/s12916-018-1175-7
Adult height and risk of 50 diseases: a combined epidemiological and genetic analysis
Abstract
Background: Adult height is associated with risk of several diseases, but the breadth of such associations and whether these associations are primary or due to confounding are unclear. We examined the association of adult height with 50 diseases spanning multiple body systems using both epidemiological and genetic approaches, the latter to identify un-confounded associations and possible underlying mechanisms.
Methods: We examined the associations for adult height (using logistic regression adjusted for potential confounders) and genetically determined height (using a two-sample Mendelian randomisation approach with height-associated genetic variants as instrumental variables) in 417,434 individuals of white ethnic background participating in the UK Biobank. We undertook pathway analysis of height-associated genes to identify biological processes that could link height and specific diseases.
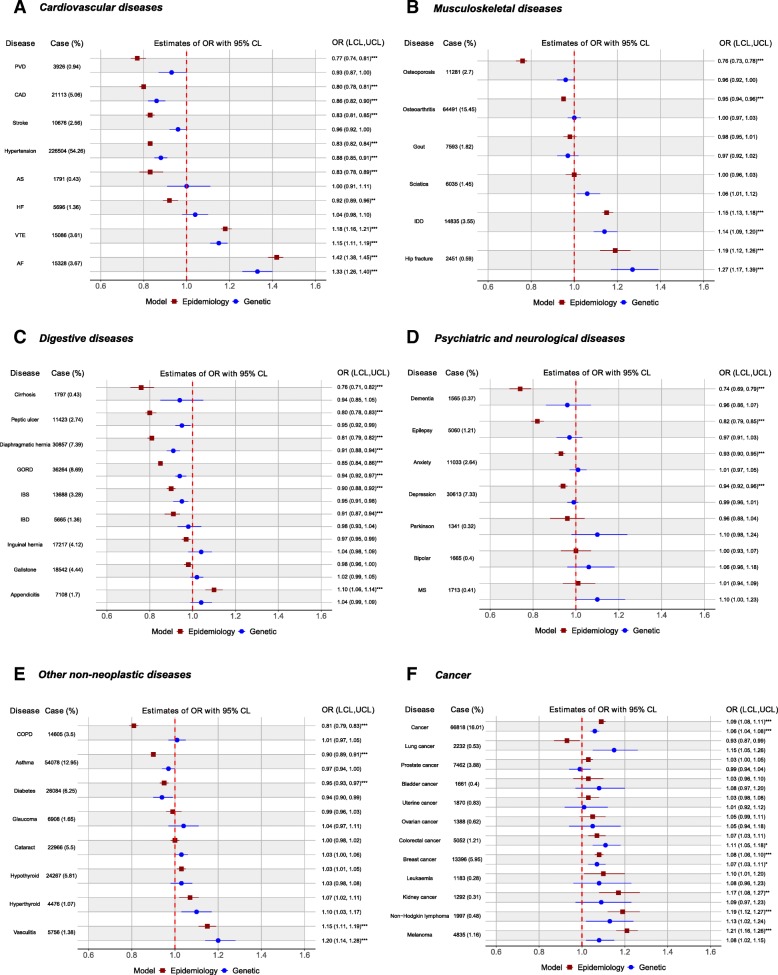
Results: Height was associated with 32 diseases and genetically determined height associated with 12 diseases. Of these, 11 diseases showed a concordant association in both analyses, with taller height associated with reduced risks of coronary artery disease (odds ratio per standard deviation (SD) increase in height ORepi = 0.80, 95% CI 0.78-0.81; OR per SD increase in genetically determined height ORgen = 0.86, 95% CI 0.82-0.90), hypertension (ORepi = 0.83, 95% CI 0.82-0.84; ORgen = 0.88, 95% CI 0.85-0.91), gastro-oesophageal reflux disease (ORepi = 0.85, 95% CI 0.84-0.86; ORgen = 0.94, 95% CI 0.92-0.97), diaphragmatic hernia (ORepi = 0.81, 95% CI 0.79-0.82; ORgen = 0.91, 95% CI 0.88-0.94), but increased risks of atrial fibrillation (ORepi = 1.42, 95% CI 1.38-1.45; ORgen = 1.33, 95% CI 1.26-1.40), venous thromboembolism (ORepi = 1.18, 95% CI 1.16-1.21; ORgen = 1.15, 95% CI 1.11-1.19), intervertebral disc disorder (ORepi = 1.15, 95% CI 1.13-1.18; ORgen = 1.14, 95% CI 1.09-1.20), hip fracture (ORepi = 1.19, 95% CI 1.12-1.26; ORgen = 1.27, 95% CI 1.17-1.39), vasculitis (ORepi = 1.15, 95% CI 1.11-1.19; ORgen = 1.20, 95% CI 1.14-1.28), cancer overall (ORepi = 1.09, 95% CI 1.08-1.11; ORgen = 1.06, 95% CI 1.04-1.08) and breast cancer (ORepi = 1.08, 95% CI 1.06-1.10; ORgen = 1.07, 95% CI 1.03-1.11). Pathway analysis showed multiple height-associated pathways associating with individual diseases.
Conclusions: Adult height is associated with risk of a range of diseases. We confirmed previously reported height associations for coronary artery disease, atrial fibrillation, venous thromboembolism, intervertebral disc disorder, hip fracture and cancer and identified potential novel associations for gastro-oesophageal reflux disease, diaphragmatic hernia and vasculitis. Multiple biological mechanisms affecting height may affect the risks of these diseases.
Keywords: Adult height; Disease risk; Genetically determined height; Instrumental variables; Mendelian randomisation.
Conflict of interest statement
Ethics approval and consent to participate
This paper is an analysis of existing data in the UK Biobank. Participants in the UK Biobank provided written consent for their data to be used for analysis. All projects submitted to and approved by the UK Biobank are subjected to their Ethics and Governance Framework.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
