

Responsiveness, Reliability, and Minimally Important and Minimal Detectable Changes of 3 Electronic Patient-Reported Outcome Measures for Low Back Pain: Validation Study
- PMID: 30355556
- PMCID: PMC6231814
- DOI: 10.2196/jmir.9828
Responsiveness, Reliability, and Minimally Important and Minimal Detectable Changes of 3 Electronic Patient-Reported Outcome Measures for Low Back Pain: Validation Study
Abstract
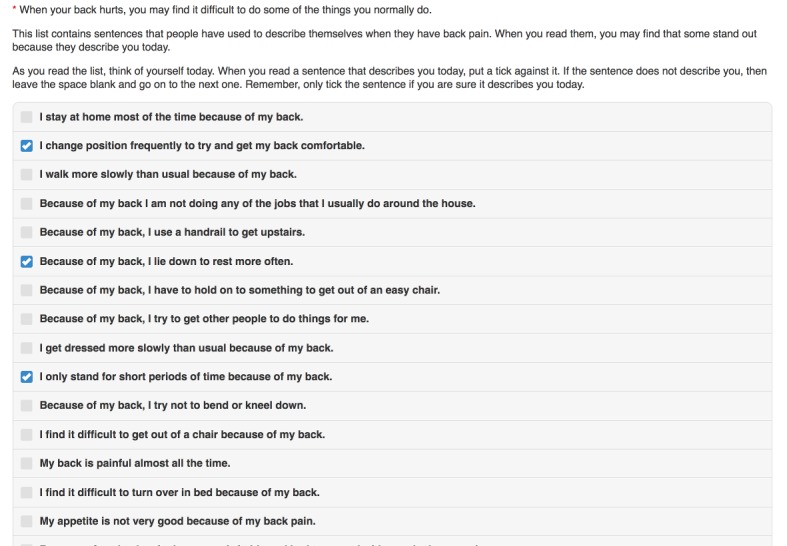
Background: The Roland Morris Disability Questionnaire (RMDQ), visual analog scale (VAS) of pain intensity, and numerical rating scale (NRS) are among the most commonly used outcome measures in trials of interventions for low back pain. Their use in paper form is well established. Few data are available on the metric properties of electronic counterparts.
Objective: The goal of our research was to establish responsiveness, minimally important change (MIC) thresholds, reliability, and minimal detectable change at a 95% level (MDC95) for electronic versions of the RMDQ, VAS, and NRS as delivered via iOS and Android apps and Web browser.
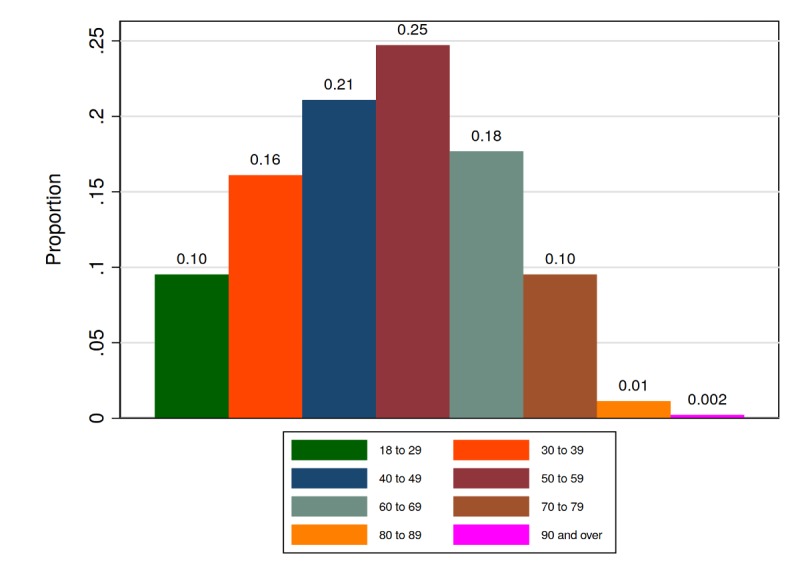
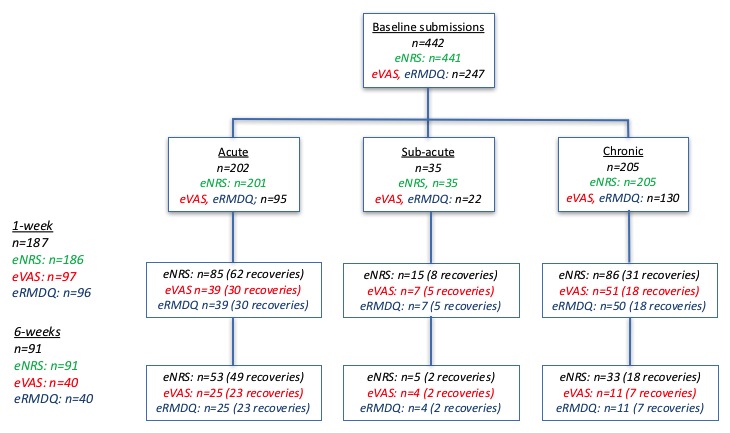
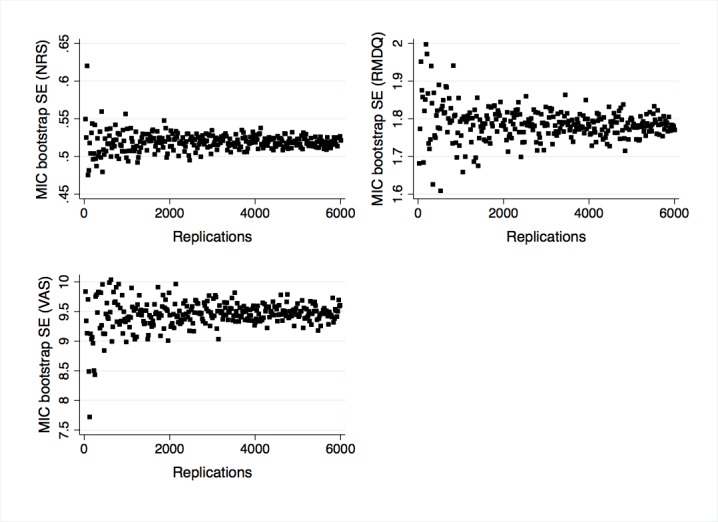
Methods: We recruited adults with low back pain who visited osteopaths. We invited participants to complete the eRMDQ, eVAS, and eNRS at baseline, 1 week, and 6 weeks along with a health transition question at 1 and 6 weeks. Data from participants reporting recovery were used in MIC and responsiveness analyses using receiver operator characteristic (ROC) curves and areas under the ROC curves (AUCs). Data from participants reporting stability were used for analyses of reliability (intraclass correlation coefficient [ICC] agreement) and MDC95.
Results: We included 442 participants. At 1 and 6 weeks, ROC AUCs were 0.69 (95% CI 0.59 to 0.80) and 0.67 (95% CI 0.46 to 0.87) for the eRMDQ, 0.69 (95% CI 0.58 to 0.80) and 0.74 (95% CI 0.53 to 0.95) for the eVAS, and 0.73 (95% CI 0.66 to 0.80) and 0.81 (95% CI 0.69 to 0.92) for the eNRS, respectively. Associated MIC thresholds were estimated as 1 (0 to 2) and 2 (-1 to 5), 13 (9 to 17) and 7 (-12 to 26), and 2 (1 to 3) and 1 (0 to 2) points, respectively. Over a 1-week period in participants categorized as "stable" and "about the same" using the transition question, ICCs were 0.87 (95% CI 0.66 to 0.95) and 0.84 (95% CI 0.73 to 0.91) for the eRMDQ with MDC95 of 4 and 5, 0.31 (95% CI -0.25 to 0.71) and 0.61 (95% CI 0.36 to 0.77) for the eVAS with MDC95 of 39 and 34, and 0.52 (95% CI 0.14 to 0.77) to 0.67 (95% CI 0.51 to 0.78) with MDC95 of 4 and 3 for the eNRS.
Conclusions: The eRMDQ was reliable with borderline adequate responsiveness. The eNRS was responsive with borderline reliability. While the eVAS had adequate responsiveness, it did not have an attractive reliability profile. Thus, the eNRS might be preferred over the eVAS for measuring pain intensity. The observed electronic outcome measures' metric properties are within the ranges of values reported in the literature for their paper counterparts and are adequate for measuring changes in a low back pain population.
Keywords: Roland Morris Disability Questionnaire; electronic patient-reported outcome measures; minimal detectable change; minimally important change; numerical rating scale; reliability; responsiveness; validation; visual analog scale.
©Robert Froud, Carol Fawkes, Jonathan Foss, Martin Underwood, Dawn Carnes. Originally published in the Journal of Medical Internet Research (http://www.jmir.org), 24.10.2018.
Conflict of interest statement
Conflicts of Interest: RF, MU, and JF are directors and shareholders of Clinvivo Ltd, the University of Warwick spin-out company that provided the software for data collection in this study. The Higher Education Innovation Funding grant paid for the development of intellectual property licensed to Clinvivo and used in this study and also paid for UK retail vouchers used as incentives to recruit participants into the study. RF and DC are nonpracticing osteopaths; CF is a practicing osteopath. MU was chair of the National Institute for Health and Care Excellence accreditation advisory committee, for which he received a fee, until March 2017. MU is chief investigator or co-investigator on multiple previous and current research grants from the UK National Institute for Health Research (NIHR), Arthritis Research UK, Arthritis Australia, and the Australian National Health and Medical Research Council. He has received travel expenses for speaking at conferences from professional organizations hosting the conferences. He is an editor of the NIHR journal series for which he receives a fee. RF and MU have published multiple papers on chronic pain, some of which are referenced in this paper. RF, MU, and JF are part of an academic partnership with Serco Ltd related to return-to-work initiatives.
Figures


References
-
- Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M, Lancet Low Back Pain Series Working Group What low back pain is and why we need to pay attention. Lancet. 2018 Mar 20;:1. doi: 10.1016/S0140-6736(18)30480-X.S0140-6736(18)30480-X - DOI - PubMed
-
- Froud R, Patterson S, Eldridge S, Seale C, Pincus T, Rajendran D, Fossum C, Underwood M. A systematic review and meta-synthesis of the impact of low back pain on people's lives. BMC Musculoskelet Disord. 2014 Feb 21;15:50. doi: 10.1186/1471-2474-15-50. https://www.biomedcentral.com/1471-2474/15/50 1471-2474-15-50 - DOI - PMC - PubMed
-
- Amundsen PA, Evans DW, Rajendran D, Bright P, Bjørkli T, Eldridge S, Buchbinder R, Underwood M, Froud R. Inclusion and exclusion criteria used in non-specific low back pain trials: a review of randomised controlled trials published between 2006 and 2012. BMC Musculoskelet Disord. 2018 Apr 12;19(1):113. doi: 10.1186/s12891-018-2034-6. https://www.biomedcentral.com/1471-2474/19/113 10.1186/s12891-018-2034-6 - DOI - PMC - PubMed
-
- Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G, COST B13 Working Group on Guidelines for Chronic Low Back Pain European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006 Mar;15 Suppl 2:S192–S300. doi: 10.1007/s00586-006-1072-1. http://europepmc.org/abstract/MED/16550448 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
