

Low-cost three-dimensional printed orbital template-assisted patient-specific implants for the correction of spherical orbital implant migration
- PMID: 30355870
- PMCID: PMC6213664
- DOI: 10.4103/ijo.IJO_472_18
Low-cost three-dimensional printed orbital template-assisted patient-specific implants for the correction of spherical orbital implant migration
Abstract
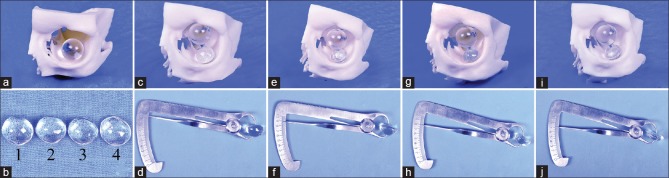
Purpose: To describe the outcomes of a patient-specific implant (PSI), fabricated using a three-dimensional (3D) printed orbital template and placed in the basin of the inferior orbital fissure to correct inferotemporally migrated spherical orbital implant.
Methods: This is a single-center, prospective, consecutive, interventional, case series of six patients, with non-porous, spherical, orbital implant migration that underwent implant recentration surgically with a novel technique. Migration was subclassified either as decentration that did not affect the prosthetic retention or as displacement that affected the prosthetic retention in the eye socket. Only implant displacements were treated. The primary outcome measure was centration of the implant clinically and radiologically, with ability to retain the prosthesis.
Results: At a mean follow-up of 21 months, all six orbital spherical implants remained centered. There were no cases of extrusion, exposure, or migration of either implants. There were no cases of PSI displacement. Additional procedures to optimize the aesthetic outcome of the customized ocular prosthesis (COP) required were simultaneous fornix formation suture in three patients, subsequent fornix formation with mucus membrane graft in two patients, and levator resection and sulcus hyaluronic acid gel injection in one patient each. The mean PSI implant weight was 2.66 ± 0.53 g. The mean COP weight was 2.2 ± 0.88 g postoperatively. The median patient satisfaction with the procedure was 9 on 10.
Conclusion: A 3D printing-assisted PSI placed in the basin of the inferior orbital fissure allows recentration of the migrated implant over a follow-up of 21 months without complications.
Keywords: Anophthalmic socket; complication; implant migration; orbital implant; three-dimensional printing.
Conflict of interest statement
There are no conflicts of interest
Figures




Comment in
-
Commentary: Using newer technology for an unresolved clinical dilemma.Indian J Ophthalmol. 2018 Nov;66(11):1607-1608. doi: 10.4103/ijo.IJO_1127_18. Indian J Ophthalmol. 2018. PMID: 30355871 Free PMC article. No abstract available.
References
-
- Custer PL, Kennedy RH, Woog JJ, Kaltreider SA, Meyer DR. Orbital implants in enucleation surgery: A report by the American Academy of Ophthalmology. Ophthalmology. 2003;110:2054–61. - PubMed
-
- Custer PL, Trinkaus KM. Porous implant exposure: Incidence, management, and morbidity. Ophthalmic Plast Reconstr Surg. 2007;23:1–7. - PubMed
-
- Sagoo MS, Rose GE. Mechanisms and treatment of extruding intraconal implants: Socket aging and tissue restitution (the “Cactus syndrome”) Arch Ophthalmol. 2007;125:1616–20. - PubMed
-
- Tao JP, LeBoyer RM, Hetzler K, Ng JD, Nunery WR. Inferolateral migration of hydrogel orbital implants in microphthalmia. Ophthalmic Plast Reconstr Surg. 2010;26:14–7. - PubMed
-
- Sundelin KC, Dafgård Kopp EM. Complications associated with secondary orbital implantations. Acta Ophthalmol. 2015;93:679–83. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
