

The Optimal Timing of Enterostomy Closure in Extremely Low Birth Weight Patients for Acute Abdomen
- PMID: 30356166
- PMCID: PMC6200749
- DOI: 10.1038/s41598-018-33351-9
The Optimal Timing of Enterostomy Closure in Extremely Low Birth Weight Patients for Acute Abdomen
Abstract
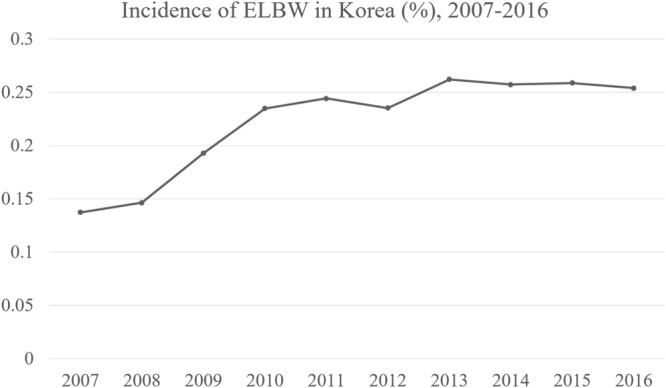
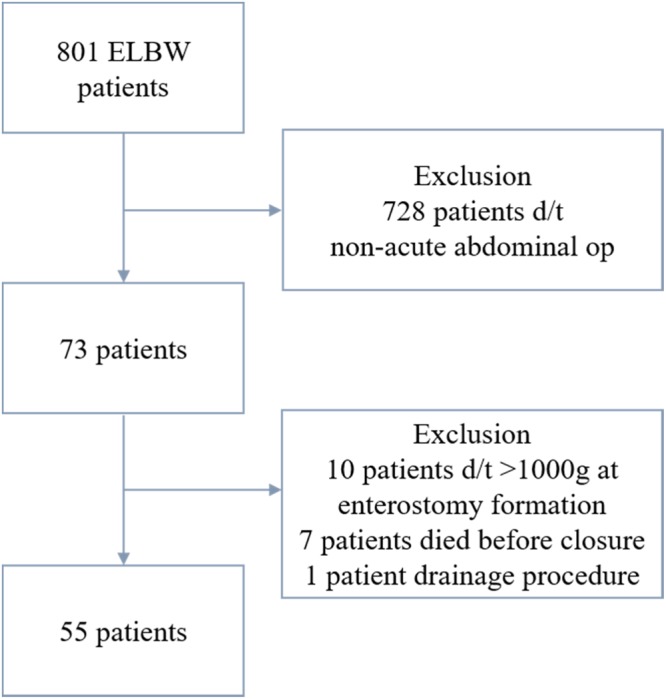
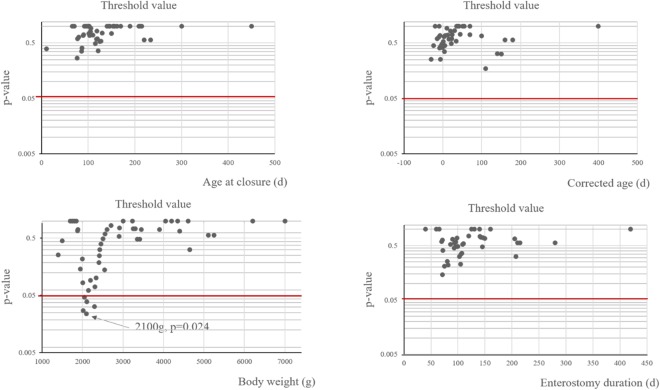
There are few reports on enterostomy closure (EC) timing for acute abdomen in extremely low birth weight (ELBW) patients. We retrospectively reviewed ELBW patients who underwent enterostomy formation (EF) and subsequent EC. We investigated baseline characteristics, surgical outcomes, and follow-up data of 55 patients and analyzed optimal timing by age at EC, enterostomy duration, and body weight (Bwt) at EC. The minimum p-value approach (MPA) using the Chi-squared test was used to determine each cut-off value. Mean gestational age was 25+3 weeks, while mean age and Bwt at EF were 10 days and 660 g. Enterostomy duration and Bwt at EC were 102 days and 2400 g. Fourteen surgical complications were related to EC. The MPA identified a cut-off of 2100 g (p = 0.039) at EC but no significant cut-off age or enterostomy duration. The 18 patients <2100 g had more enterostomy-related problems at EC than the >2100 g group (66.7% vs 10.8%, p < 0.001). No other characteristics were significantly different. Operation time, ventilator period, hospital stay, parenteral nutrition duration, and full feeding day were significantly longer in <2100 g patients. Follow-up Bwt did not differ (11.55 kg vs 13.95 kg, p = 0.324). Our findings suggest EC can be safely performed when Bwt is over 2100 g.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Moon JY, Hahn WH, Shim KS, Chang JY, Bae CW. Changes of Maternal Age Distribution in Live Births and Incidence of Low Birth Weight Infants in Advanced Maternal Age Group in Korea. Korean J Perinatol. 2011;22:30–36.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
