

Profibrotic, Electrical, and Calcium-Handling Remodeling of the Atria in Heart Failure Patients With and Without Atrial Fibrillation
- PMID: 30356673
- PMCID: PMC6189336
- DOI: 10.3389/fphys.2018.01383
Profibrotic, Electrical, and Calcium-Handling Remodeling of the Atria in Heart Failure Patients With and Without Atrial Fibrillation
Abstract
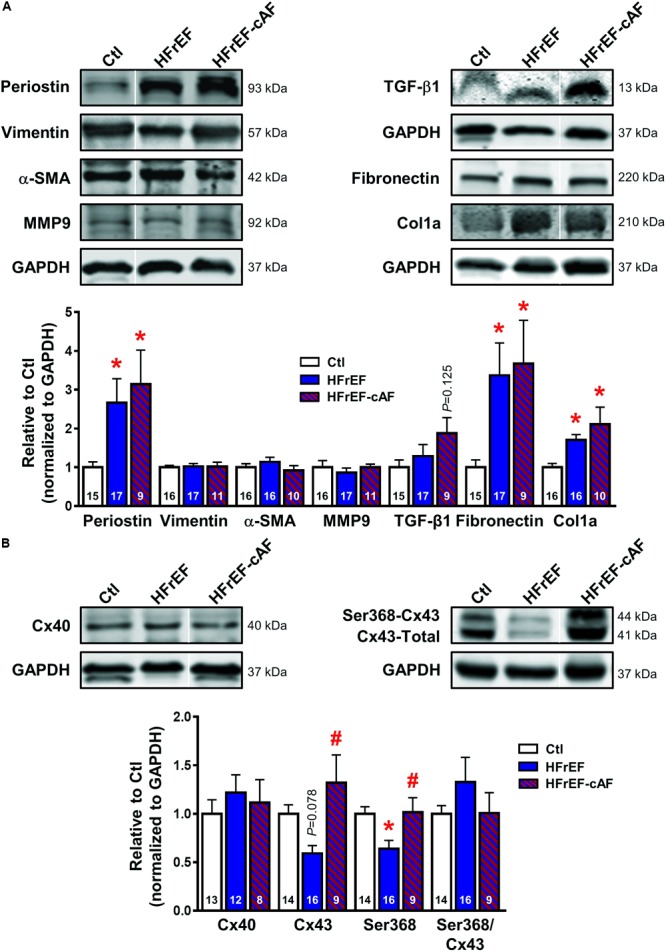
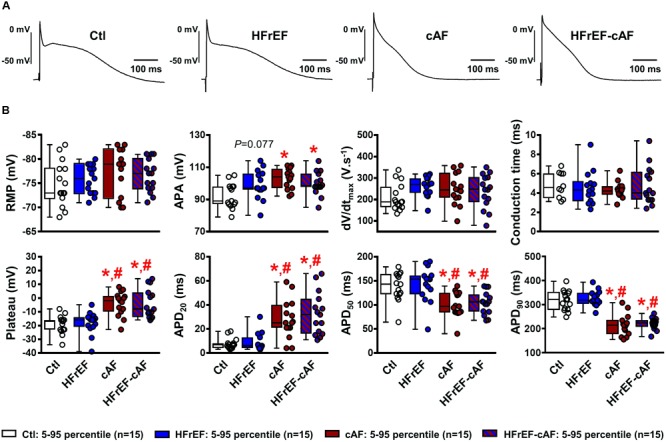
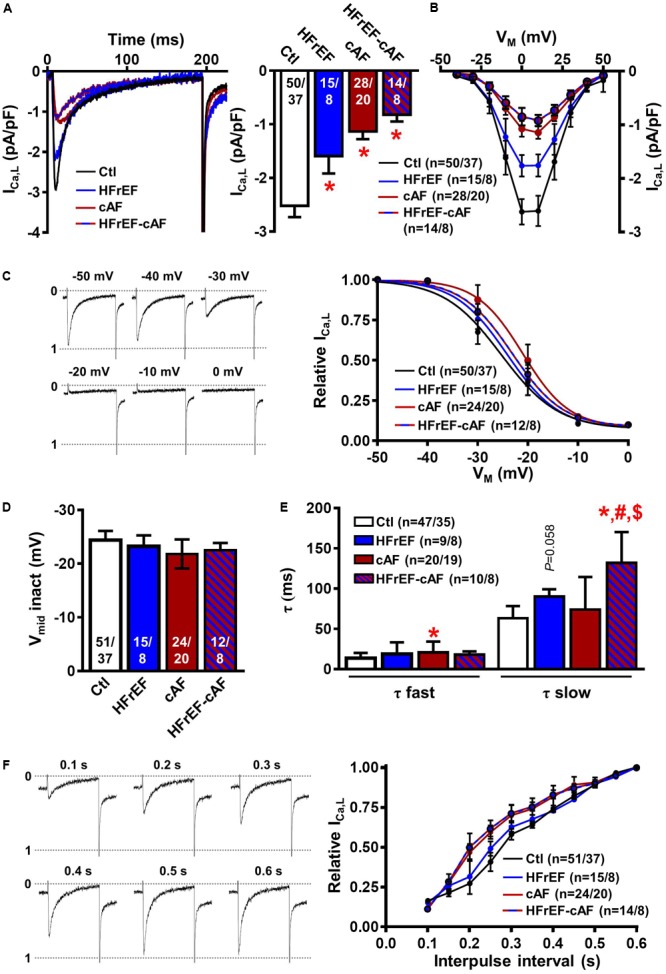
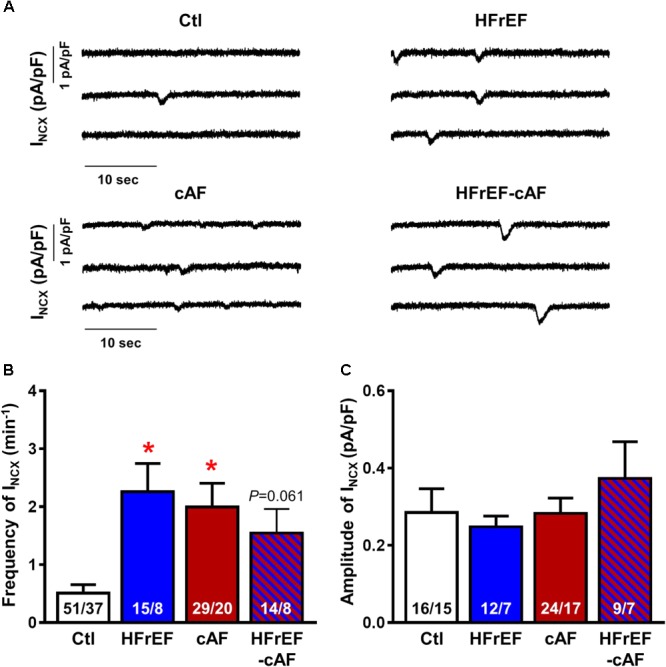
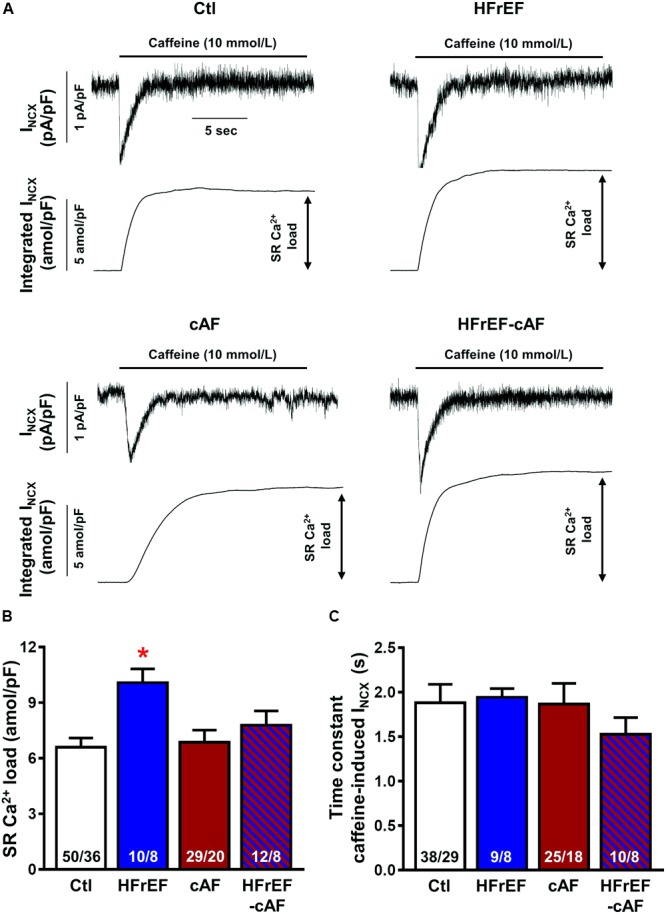
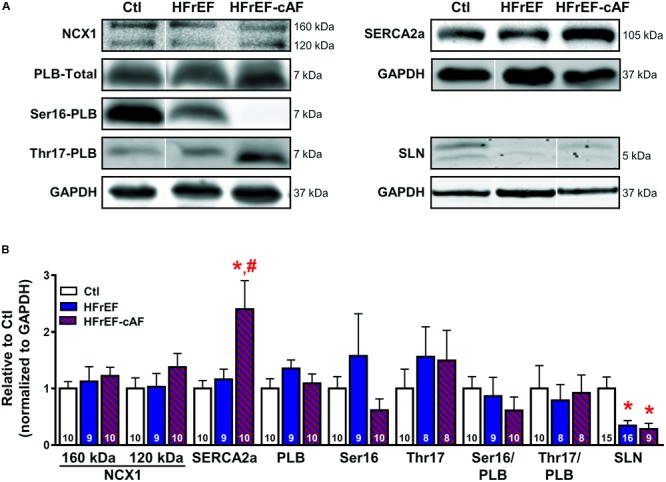
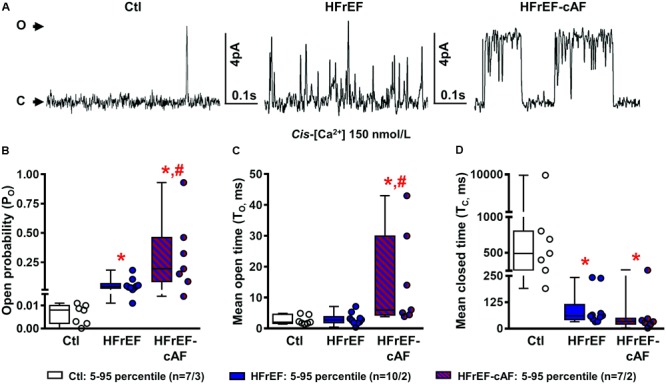
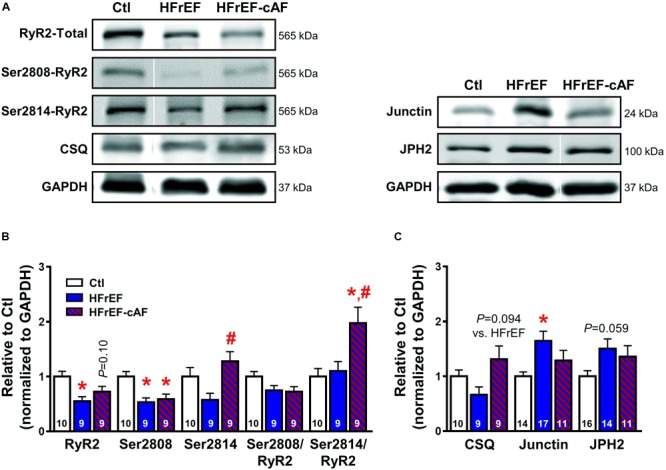
Atrial fibrillation (AF) and heart failure (HF) are common cardiovascular diseases that often co-exist. Animal models have suggested complex AF-promoting atrial structural, electrical, and Ca2+-handling remodeling in the setting of HF, but data in human samples are scarce, particularly regarding Ca2+-handling remodeling. Here, we evaluated atrial remodeling in patients with severe left ventricular (LV) dysfunction (HFrEF), long-standing persistent ('chronic') AF (cAF) or both (HFrEF-cAF), and sinus rhythm controls with normal LV function (Ctl) using western blot in right-atrial tissue, sharp-electrode action potential (AP) measurements in atrial trabeculae and voltage-clamp experiments in isolated right-atrial cardiomyocytes. Compared to Ctl, expression of profibrotic markers (collagen-1a, fibronectin, periostin) was higher in HFrEF and HFrEF-cAF patients, indicative of structural remodeling. Connexin-43 expression was reduced in HFrEF patients, but not HFrEF-cAF patients. AP characteristics were unchanged in HFrEF, but showed classical indices of electrical remodeling in cAF and HFrEF-cAF (prolonged AP duration at 20% and shorter AP duration at 50% and 90% repolarization). L-type Ca2+ current (ICa,L) was significantly reduced in HFrEF, cAF and HFrEF-cAF, without changes in voltage-dependence. Potentially proarrhythmic spontaneous transient-inward currents were significantly more frequent in HFrEF and HFrEF-cAF compared to Ctl, likely resulting from increased sarcoplasmic reticulum (SR) Ca2+ load (integrated caffeine-induced current) in HFrEF and increased ryanodine-receptor (RyR2) single-channel open probability in HFrEF and HFrEF-cAF. Although expression and phosphorylation of the SR Ca2+-ATPase type-2a (SERCA2a) regulator phospholamban were unchanged in HFrEF and HFrEF-cAF patients, protein levels of SERCA2a were increased in HFrEF-cAF and sarcolipin expression was decreased in both HFrEF and HFrEF-cAF, likely increasing SR Ca2+ uptake and load. RyR2 protein levels were decreased in HFrEF and HFrEF-cAF patients, but junctin levels were higher in HFrEF and relative Ser2814-RyR2 phosphorylation levels were increased in HFrEF-cAF, both potentially contributing to the greater RyR2 open probability. These novel insights into the molecular substrate for atrial arrhythmias in HF-patients position Ca2+-handling abnormalities as a likely trigger of AF in HF patients, which subsequently produces electrical remodeling that promotes the maintenance of the arrhythmia. Our new findings may have important implications for the development of novel treatment options for AF in the context of HF.
Keywords: Ca2+ handling; atrial fibrillation; heart failure; heart failure with reduced ejection fraction; human atrial cardiomyocytes.
Figures
References
-
- Brundel B. J., Henning R. H., Kampinga H. H., Van Gelder I. C., Crijns H. J. (2002). Molecular mechanisms of remodeling in human atrial fibrillation. Cardiovasc. Res. 54 315–324. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous