

Atherosclerosis Might Be Responsible for Branch Artery Disease: Evidence From White Matter Hyperintensity Burden in Acute Isolated Pontine Infarction
- PMID: 30356780
- PMCID: PMC6189443
- DOI: 10.3389/fneur.2018.00840
Atherosclerosis Might Be Responsible for Branch Artery Disease: Evidence From White Matter Hyperintensity Burden in Acute Isolated Pontine Infarction
Abstract
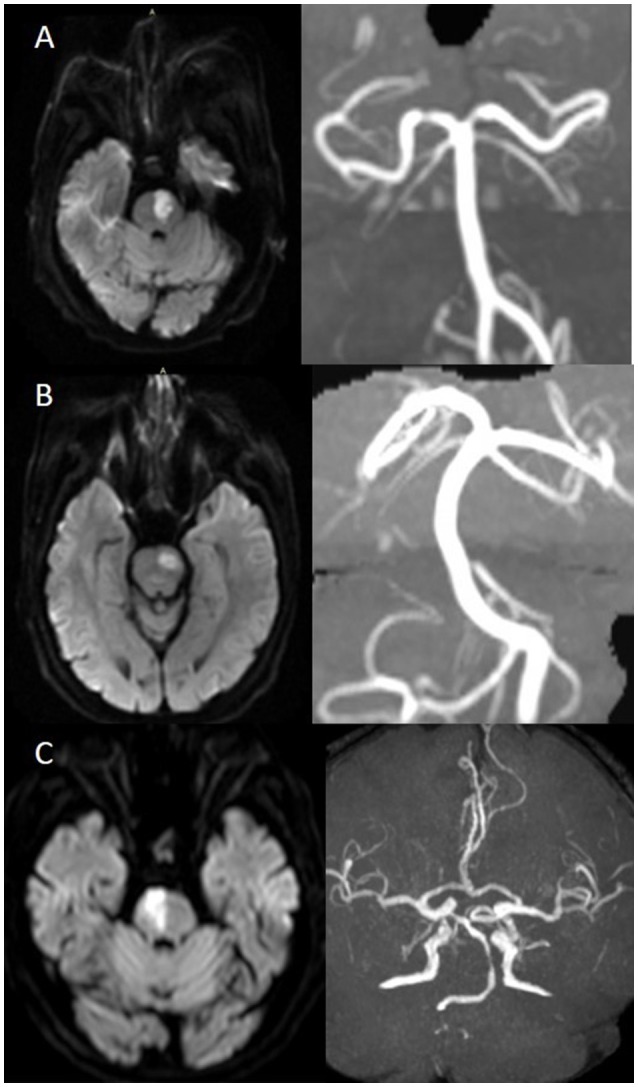
Objective: To investigate an MRI-based etiological classification for acute isolated pontine infarcts and to assess differences in vascular risk factors, clinical characteristics and WMH burden among the etiological subtypes. Methods: All participants from SMART cohort with DWI-proven acute isolated pontine infarcts (AIPI) were included and categorized into 3 groups: large-artery-occlusive disease (LAOD), basilar artery branch disease (BAD), and small vessel disease (SVD), according to basilar artery atherosclerosis severity and lesion extent of the transverse axial plane. The vascular risk factors and 6-month functional outcome was analyzed among 3 groups. Results: Of the 1129 patients enrolled, 175 had AIPI. BAD was the most frequent subtype of AIPI (46.3%), followed by SVD (36.0%) and LAOD (17.7%). Neurological impairment on admission was more severe in the LAOD group, followed by BAD. The BAD group had greater frequencies of female sex, hypertension, diabetes mellitus compared to the SVD group (P < 0.05). NIHSS on admission were significantly higher in the BAD group as compared with the SVD group (P < 0.001), but no difference was found between BAD and LAOD group. Poor outcome (mRS≥3) was found in only 13.7% of patients at 6-month post-stroke and there was no difference among 3 groups. WMH severity was significant higher in the SVD group compared to the BAD group for the deep subcortical region; however, there was no difference for the periventricualr region. There was no significant difference in either DWMH or PVWMH severity between the BAD and LAOD groups. Conclusion: BAD is the most frequent etiology of AIPI followed by SVD and LAOD. WMH burden, vascular risk factors and clinical characteristics in BAD group were more similar to the LAOD group, rather than to the SVD group, suggesting the atherothrombotic nature of BAD.
Keywords: SMART study; branch atherosclerotic disease; etiological classification; isolated pontine infarction; white matter hyperintensity.
Figures
References
LinkOut - more resources
Full Text Sources
Medical
Research Materials